Apocrine Hidrocystoma of the Cheek
Article information
Apocrine hidrocystomas commonly occur as a solitary cystic lesions and are very frequently located near the eye. They are thought to be benign skin neoplasms derived from the secretory portion of the apocrine gland and usually present as a superficial, solitary, various-colored (skin-colored, light-brown, red-brown, bluish, or black) nodule on the periorbital area of the mid dermis layer [1]. It is interesting to note that whereas the axilla and the periorbital region are considered to be the most common sites of origin of apocrine hidrocystomas, the apocrine glands are usually located in the chest or perineumand only very rarely are located in the facial area [1]. So far, a total of 167 cases of apocrine hidrocystoma have been reported and systematically organized in Japan [2]. However, since the first report occurring on vagina of a 31-year-old female, only a few cases have been reported in Korea [3-5]. We, therefore, report a rare case of apocrine hidrocystoma occurring on the cheek in a 58-year-old female with a literature review.
A 58-year-old woman presented with a 10-year history of a painless mass on her right cheek. She had no notable past or family history except antihypertensive drug medication for hypertension. It had never bled or been infected. She had not noticed any increase in size with temperature or seasonal variation. The physical examination showed a mass measuring 15×15 mm on her cheek. The overlying skin was intact and the mass was smooth surfaced, dome shaped, and deep purple-colored (Fig. 1A). She was bothered by the mass only from a cosmetic point of view. Sonographically, a well-circumscribed cystic lesion measuring 13×15 mm was identified. However, there was no connection with any other adjacent structure (Fig. 1B). It was removed under local anesthesia. There was a distinct plane of dissection. Healing was uneventful. Macroscopic examination revealed a cyst of 18×15×12 mm in size, containing brownish, slimy fluid. The histopathologic examination showed cystic spaces in the subcutaneous layer (Fig. 2A). On microscopic examination, the dermis contained a multilocular cyst, lined by a cylindric epithelium of the apocrine secretory type. Beneath this was an outer layer of myoepithelial cells. The inner epithelial lining of the cyst was composed of columnar cells with eosinophilic cytoplasm and basally-located nuclei showing a "decapitation" secretion indicative of apocrine secretion (Fig. 2B, C). These histologic features are characteristic of apocrine hidrocystoma. A faint scar remained on her cheek at her two-month follow-up visit.
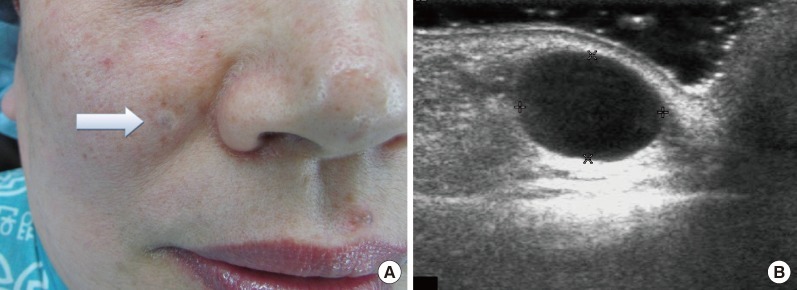
(A) A dome-shaped, deep purple cystic mass (white arrow) on the right cheek. (B) A well-circumscribed cystic lesion without any other adjacent structure invasion, measuring 13×15 mm was identified sonographically.
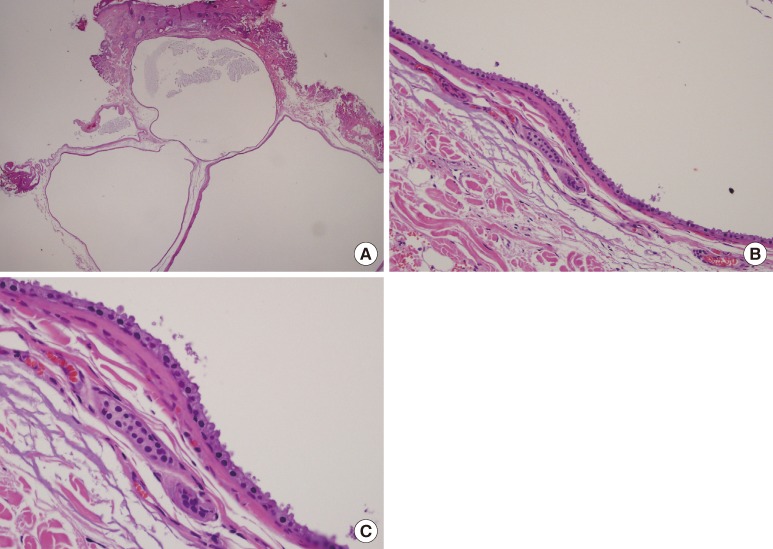
Histological study. (A) Overview of the apocrine hidrocystoma with a multilocular cystic space (H&E, ×40). (B) Lining of cysts with an inner layer of apocrine cells and an outer layer of myoepithelial cells (H&E, ×100). (C) A row of secretory cells which show decapitation (H&E, ×200).
Apocrine hidrocystomas are benign cystic tumors that arise from the apocrine secretory coli. Though there are some references to multiple apocrine hidrocystomas in the literature, the most common presentation is a solitary lesion which is very frequently located near the eye. The incidence may not be known accurately, but it is estimated that it may be one per thousand of submitted cutaneous biopsies. However, presumed apocrine hidrocystomas located on the inner or outer canthus of the lower eyelid have the possibility of being Moll's gland cysts [1]. Therefore, we can conclude the true incidence of apocrine hidrocystoma on the face may be lower than reported.
Solitary apocrine hidrocystomas have no seasonal variations, but multiple lesions have seasonal variations like eccrine hidrocystomas, which tend to appear more in hot and humid weather. Histologically, they are characterized by unilocular or multilocular cysts that are lined by a double lining of epithelium with the outer layer comprising flat myoepithelial cells and inner layer containing large columnar or cuboidal cells with eosinophilic cytoplasm and round or oval vesicular nuclei at the base of these cells. Decapitation secretion is a hallmark of apocrine hidrocystoma. A simple needle puncture is often done for a solitary lesion of hidrocystoma. It is also easily treated with simple excision [2-5].
According to the Japanese literature, locations of lesions of apocrine hidrocystomas in Japan were face (61.1%), scalp (12.6%), trunk (13.7%), and extremities (12.0%). The tumor seems to occur evenly in any age group, and in only 15 cases (9.0%) was the tumor found in apocrine gland-bearing regions, such as the axilla and groin [2]. However, we do not have properly compiled disease statistics in Korea. Among the papers that have been published in Korea to date, cases in the axilla and groin areas have not even been reported. The genital area, anterior chest wall, and eyelids were the only places. Considering the possibility of Moll's gland cysts, we can assume that only a few cases of apocrine hidrocystomas have been identified for certain in Korea so far (Table 1) [2-5]. This is a very small number of cases compared to Japan. In light of this disparity, we propose that the Korean medical community should systematize and strengthen the reporting system for not only this, but every disease, in order to generate more accurate medical statistics.

Literature review of apocrine hidrocystomas reported in Korea
Notes
No potential conflict of interest relevant to this article was reported.