Aesthetic Refinement of the Dog Ear Correction: The 90° Incision Technique and Review of the Literature
Article information
The closure of any circular or asymmetric wound results in puckering or excess of tissue known as dog ears. Tissue dynamics, wound geometry, surface contour, and surgical technique affect dog ear formation [1,2]. Despite good preoperative planning for skin management techniques including Burow's triangle, V-Y advancement flap, M-plasty [3], and S-plasty [4], and despite following intraoperative procedures including proper undermining of a shallow wound, proper 90° angle of the scalpel blade, precise suture placement, and removal of excess underlying fat, sometimes a dog ear occurs anyhow. Methods for correcting dog ears include excision of the excess tissue in the shape of a triangle, crescent or ellipse; excision of conical folds of tissue at the end of the wound in the same direction as the long axis of the original wound; and excision of the dog ear at a 120° angle to the long axis of the existing excision line in a shape resembling a hockey stick [5]. They are extensively described in the literature, but they all lead to wound extension. Only M-plasty allows for reduction in the scar's length but produces a double-tailed scar, so if the total length with the two tails is considered, the new scar is still longer than the original one. We have developed a new and easy technique for dog ear correction without extending the length of the original wound.
To remove a dog ear, the wound should be sutured until the elevation becomes pronounced. A hook placed in the end of the wound defines the extent of the dog ear. The elevation is then excised by creating a 90° incision at the end of the wound where the dog ear appears. In this way, a small triangular advancement flap can be raised upward or downward according to the skin region desired to be removed. This flap is brought across the wound so that the skin excess can be cut straightforwardly. A portion of the flap is then removed to the extent required and the 90° incision created will disappear as well (Figs. 1, 2).
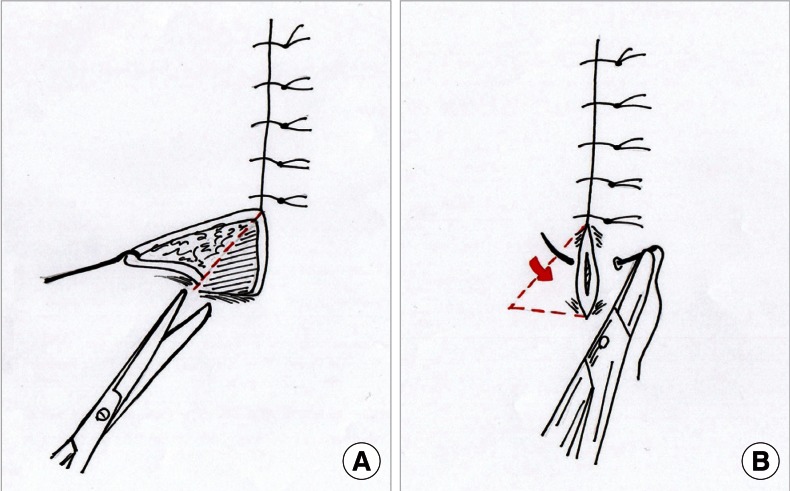
The schema of our new technique for correcting a dog ear at the end of a wound. (A) Incision at a 90° angle to the long axis of the existing excision line to create a triangular advancement skin flap downward. As much of the triangular raised flap is removed as the correction requires. (B) The 90° incision created disappears as soon as the skin has been sutured. The steep protrusion of the dog ear disappears without either lengthening the wound or creating new scars. The red arrow shows the direction of the flap advancement used for dog ear removal.
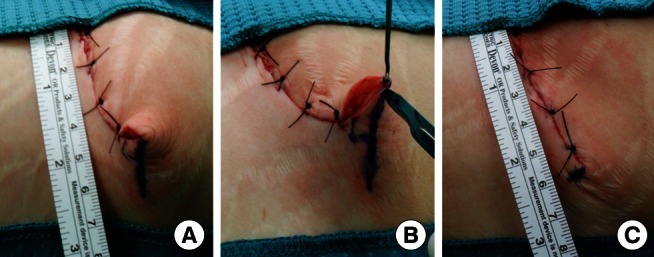
Sequenced images of the 90° incision technique. (A) With an ink pen, a line is drawn at 90° along the base on one side of the standing full cone dog ear. (B) The apex of the dog ear is elevated with a skin hook. The line will be then incised, thus creating a triangular flap ready for removal. (C) After the triangular skin flap has been removed, the dog ear disappears without lengthening the wound.
The 90° incision technique enables correction of a dog ear without either lengthening the wound or creating new scars, thus improving the aesthetic outcome of the procedure.
Notes
No potential conflict of interest relevant to this article was reported.