The Correction of a Secondary Bilateral Cleft Lip Nasal Deformity Using Refined Open Rhinoplasty with Reverse-U Incision, V-Y Plasty, and Selective Combination with Composite Grafting: Long-term Results
Article information
Abstract
Background
This article presents long-term outcomes after correcting secondary bilateral cleft lip nasal deformities using a refined reverse-U incision and V-Y plasty or in combination with a composite graft in order to elongate the short columella.
Methods
A total of forty-six patients underwent surgery between September 1996 and December 2008. The age of the patients ranged from 3 to 19 years of age. A bilateral reverse-U incision and V-Y plasty were used in 24 patients. A composite graft from the helical root was combined with a bilateral reverse-U incision in the 22 patients who possessed a severely shortened columella. The follow-up period ranged between 2 and 10 years.
Results
A total of 32 patients out of 46 were evaluated postoperatively. The average columella length was significantly improved from an average of 3.7 mm preoperatively to 8.5 mm postoperatively. The average ratio of the columella height to the alar base width was 0.18 preoperatively and 0.29 postoperatively. The postoperative basal and lateral views revealed a better shape of the nostrils and columella. The elongated columella, combined with a composite graft, presented good maintenance of the corrected position with no growth disturbance. A composite graft showed color mismatching in several patients. Twenty-six patients demonstrated no alar-columella web deformity and satisfactory symmetry of the nostrils. Four patients experienced a drooping and overhanging of the corrected alar-columella web.
Conclusions
A bilateral reverse-U incision with V-Y plasty or in combination with a composite graft was effective in correcting secondary bilateral cleft lip nasal deformity.
INTRODUCTION
Typical secondary bilateral cleft lip nasal deformities present a short columella, a laterally-spreading dome of the alar cartilages resulting in a bifid and drooping nose tip, the laterally displaced alar bases resulting in a flaring alar-facial angle and a broadened nose floor, hypoplasia of bilateral pear-shaped nostrils, and almost no nasolabial angle in profile [1]. The fundamental components of the surgical correction of a bilateral cleft lip nasal deformity include the repositioning of the cleft lower lateral cartilage to a more normal anatomic position, achieving a symmetrical projection of both alar domes, elongating the columella, and moving the cleft alar base medially so as to obtain symmetry of the nasal floor.
Correcting a bilateral cleft lip nasal deformity is a challenge due to its complex nature. Many different techniques have been used over the years to correct such deformities [2-11]. The "short columella" is the hallmark of the bilateral cleft lip nasal deformity. Methods of elongating the columella have served as the basis for the secondary correction of the bilateral cleft lip nose [8-11]. However, with tissue deficiency or scar contracture on the upper lip, it is very difficult to achieve a good nasal profile with conventional methods. Composite grafts from a distant area can be used to elongate the short columella in a bilateral cleft lip nasal deformity [2,10,11].
The reverse-U incision has been used to correct a secondary unilateral or bilateral cleft lip nasal deformity by itself or in combination with open rhinoplasty incision [3-7]. The current author has modified and refined the reverse-U incision for the correction of the secondary unilateral cleft lip nasal deformity. This was expected for ten years so as to avoid unsatisfactory results [11,12]. In addition, the current author has applied the proposed technique of open rhinoplasty with refined bilateral reverse-U incision for the correction of bilateral cleft lip nasal deformity. There are no reports in the literature on correction of bilateral cleft nasal deformity with severe short columella treated using bilateral reverse-U incision and V-Y plasty in combination with a composite graft.
In the present study, we report the long-term surgical results of correction of a secondary bilateral cleft lip nasal deformity using a refined bilateral reverse-U incision and V-Y plasty or in combination with a composite graft, based on an average of 5 years of follow-up.
METHODS
A total of 46 patients with secondary bilateral cleft lip nasal deformities underwent surgery between September 1996 and December 2008. The age of the patients ranged between 3 and 19 years of age. Twenty-six were male and twenty were female. The analysis of the nasal profile was performed with the following landmarks: pronasale, columella peak, subnasale (the midpoint of the columella base at the apex of the angle), and alar curvature point. The measurement was done with a real-size digital photograph of the worm's-eye view prior to the operation and at the time of the final follow-up visit. Nasal profiles were evaluated with the columellar height (the distance from the columella peak to the subnasale), the ratio of columellar height to nasal height (the distance from the pronasale to the subnasale), the ratio of columellar height to alar base width (the distance from the alar curvature point to the contralateral alar curvature point) (Fig. 1).
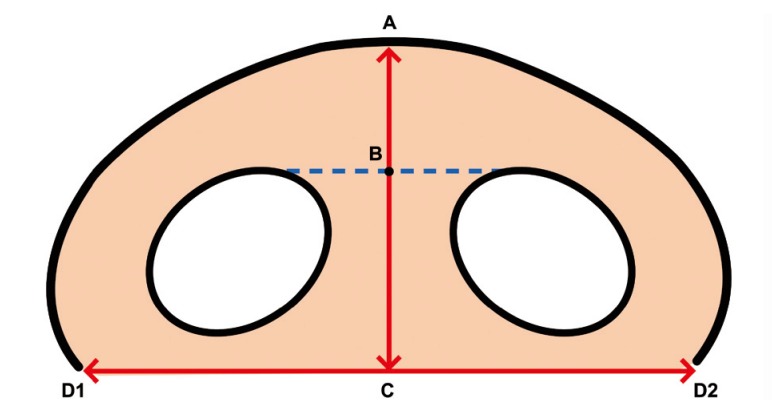
Evaluation of nasal profiles
Nasal profiles were evaluated by the columellar height (B-C, the distance from the columellar peak to the subnasale), the ratio of columellar height to nasal height (A-C, the distance from the pronasale to the subnasale), the ratio of columellar height to alar base width (D1-D2, the distance from the alar curvature point to the contralateral alar curvature point). (A means pronasale. B means columella peak. C means subnasale. D means alar curvature point.)
Surgical techniques
To maintain adequate hemostasis, 1% lidocaine in a solution of 1:100,000 epinephrine is infiltrated over the dorsum of the nose, nasal tip, columella, and nasal dorsum depending on the area to be corrected. In addition, the nose is packed with 1 cm gauze which has been soaked in epinephrine solution for several minutes.
Open rhinoplasty with a bilateral reverse-U incision was modified according on the length of the columella in the bilateral cleft lip nasal deformity. In the case of a mildly short columella, a reverse-U incision and V-Y plasty are combined with an open rhinoplasty incision (Fig. 2). The reverse-U incision is continued to a transcolumellar incision at the columella base. The degloving procedure begins at the bottom of the transcolumellar incision. The columellar flap is raised and, as a result, the lower and upper lateral cartilages are both exposed (Fig. 3). The areolar tissue between the lower lateral cartilages is elevated with the dorsal skin. Any loose fatty and connective tissue is preserved as much as possible. The abnormal lateral crus is severed from its lateral attachment. A V-shaped incision is made at the base of the cleft ala. A V-shaped incision is made continuous with the lateral end of the reverse-U incision. Through this incision, using a small curved Metzenbaum scissors, the cleft lower lateral cartilage is exposed, and then dissected completely to its junction with the medial crus, including the mucosal lining. The alar base is then freed from the piriform aperture and the mucoperichondrial flap is then transposed medially in order to create symmetry of the nasal floor and nostril. The soft tissue in the alar-columellar web, adjacent to the nasal mucosa of the reverse-U flap, is trimmed to facilitate redraping into the nasal cavity. Using a No. 15 blade, two to three fine scores were made in the soft tissue of the alar-columellar web adjacent to the nasal mucosa of the reverse-U flap. One horizontal mattress suture, using 6-0 Vicryl, is placed on the scored area of the reverse-U flap to create a concave shape for easy redraping into the concave nasal surface (Fig. 3B).

Schematic diagram of the incisions
A schematic diagram of the incisions of open rhinoplasty with a bilateral reverse-U incision and V-Y plasty. (A) Open rhinoplasty with a bilateral reverse-U incision and V-Y plasty. (B) Open rhinoplasty with a bilateral reverse-U incision and V-Y plasty in combination with composite graft from the helix in a short columella.
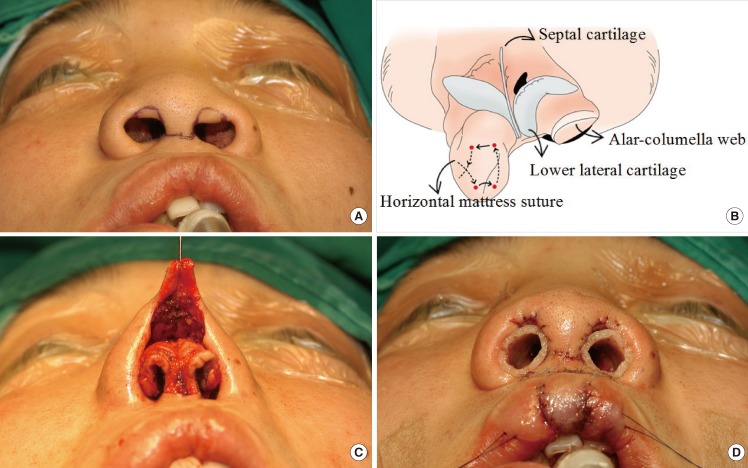
Operative technique
(A) A preoperative design. (B) After exposure of both lower lateral cartilages, the alar-columellar web is present on the left nostril. On the right nostril, the soft tissue in the alar-columellar web which neighbours the nasal mucosa of the reverse-U flap was trimmed. Horizontal mattress suture on the scored area of the reverse-U flap that modifies the concave shape for easy redraping into the concave nasal surface. (C) Both lower lateral cartilages were fixed together to elevate the nasal tip. (D) Immediate postoperative view with internal nasal retainer.
Both lower lateral cartilages are fixed together using 5-0 white nylon to elevate the nasal tip (Fig. 3C). The mucoperichondrial flap is then advanced medially and superiorly into a more favorable position. The reverse-U flap is rotated along the reverse-U incision. The defect in the mucosa is repaired with a V-Y closure after the advancement of the lateral crus. Occasionally, the rotated reverse-U flap needs to be trimmed to create symmetric nostrils. The alar transfixion sutures [13] are placed in the vestibular skin to avoid dead space between the skin and the repositioned cleft lower lateral cartilages. A 5-0 polydioxanone (PDS) suture is passed from the inside to the outer surface of the ala by using the tips of the forceps. The suture is then returned through the outer suture hole and back into the inner aspect of the vestibular skin where it is tied as a mattress subcuticular suture. Usually, two or three sutures are needed.
In the case of wide nostrils, after redraping the nasal skin, the widened alar base is corrected using alar base advancement. The bilateral subcutaneous tissue of the alar base is tethered with 4-0 white nylon to cinch the alar bases, thus narrowing the alar flares.
In the case of a severely short columella, open rhinoplasty with a bilateral reverse-U incision is used (Fig. 2B). The degloving procedures begins at the bottom of the transcolumellar incision. The columellar flap is raised, and both lower lateral cartilages are exposed. Both mucochondrial flaps are advanced and fixed to the lower lateral cartilages. Interdomal sutures are performed to prevent nasal tip bulging. If there is insufficient projection of the nasal tip after mobilization of the cleft lower lateral cartilages, conchal cartilage onlay-grafting is performed to augment the nasal tip in the adult. To correct a short columella, a 5- to 10-mm composite wedge-shaped graft donated from the root of the helix is used. The donor defect is closed primarily. The cartilaginous portion of the composite graft is then used as structural support for the columella. The skin portion of the composite graft is used to lengthen the short columella. The composite tissue is sutured to restore the lining of the columellar skin and nasal mucosa.
A homemade nasal retainer is then applied at least for six months in order to maintain the corrected nostril contour and to prevent the nostril from deforming (Fig. 3D).
Statistical analysis
Statistical analysis was performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The paired t-test was used to compare the preoperative and postoperative measurements in the two groups. Values of P<0.05 were accepted as significant.
RESULTS
A composite graft was combined with a bilateral reverse-U incision in 22 patients with a short columella. There was no necrosis of the composite graft. Alar base advancement was conducted in 21 patients with wide nostrils. A cancellous iliac bone graft for an alveolar cleft was performed in ten patients between the ages of 9 and 11. Onlay-graft of the conchal cartilage was performed to augment the nasal tip in 4 adults. The follow-up period ranged from 2 to 10 years, with an average of 5 years.
A total of 32 patients among 46 patients were evaluated (Table 1). The average columellar height was significantly improved from 3.7±2.1 mm (range, 1.6 to 5.8 mm) preoperatively to 8.5±1.2 mm (range, 7.3 to 9.7 mm) postoperatively, with a statistical significance of P<0.05. The ratio of columellar height to nasal height was 0.28±0.05 preoperatively and 0.51±0.02 postoperatively. The reference value in normal Korean people is 0.52±0.07 [14,15]. The ratio of columellar height to alar base width was 0.18±0.05 preoperatively and 0.29±0.05 postoperatively. The reference value in normal Korean people is 0.31±0.06 [14,15]. Preoperative depressed nasal tip and flaring of the nasal apertures were corrected in all patients (Figs. 4-7). The postoperative frontal views showed better projection of the alar domes and correction of the laterally displaced alar bases. The elongated columella, combined with a composite graft, presented good maintenance of the corrected position with no growth disturbance (Fig. 7). A composite graft, however, showed color mismatching in several patients.
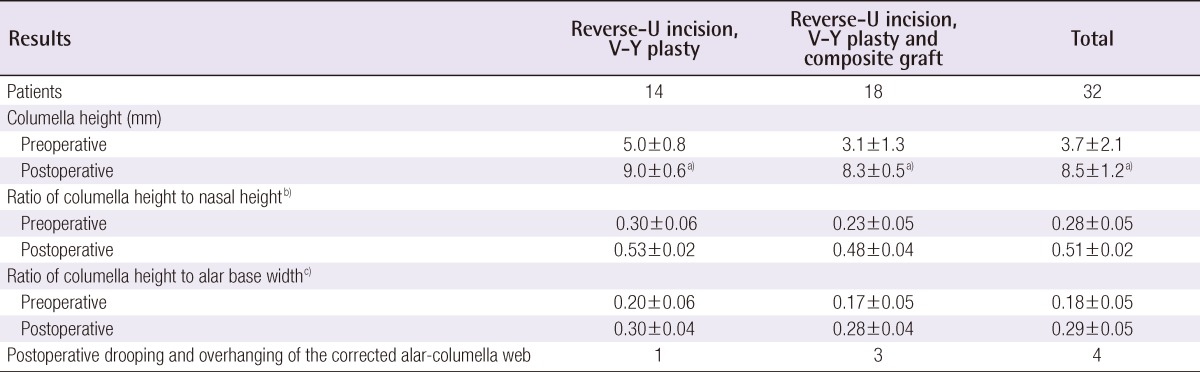
Comparison between preoperative and postoperative nasal profiles according to surgical method
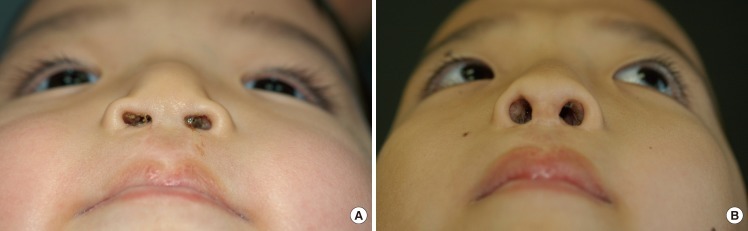
A 15-year-old boy with a bilateral cleft lip nasal deformity
A 15-year-old boy with a bilateral cleft lip nasal deformity corrected by open rhinoplasty with a bilateral reverse-U incision combined with V-Y plasty. (A) Preoperative view. (B) Five-year postoperative view.

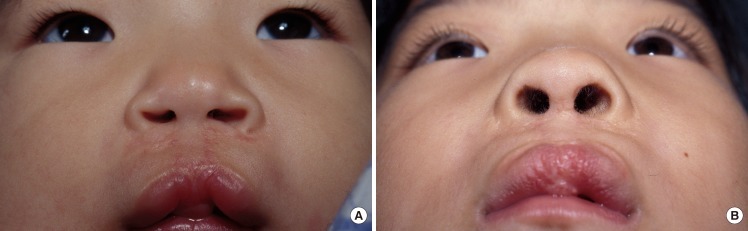
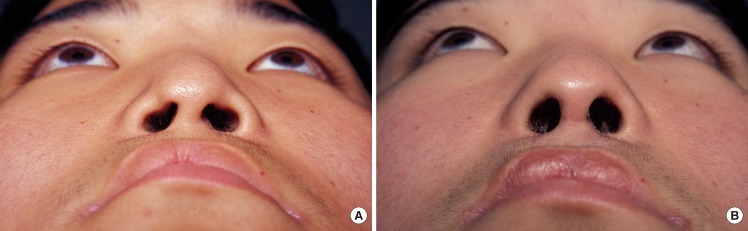
A 5-year-old girl with a bilateral cleft lip nasal deformity with a short columella
A 5-year-old girl with a bilateral cleft lip nasal deformity with a short columella corrected by open rhinoplasty with a bilateral reverse-U incision and V-Y plasty combined with a composite graft. (A) Preoperative view. (B) Composite graft from helix. (C) Ten-year postoperative view.
Twenty-eight patients among 32 patients demonstrated no alar-columellar web deformity and satisfactory symmetry of the nostrils. In addition, there was no overhanging excess skin in the superomedial nostril rim, and the contour of the alar rim was natural and slender. Four patients experienced a drooping and overhanging of the corrected alar-columellar web. Possible causes of redrooping included the undercorrection of the vestibular web or an incomplete redraping of the reverse-U flap into the concave nasal surface. Consistent application of a nasal retainer is important to maintain the corrected alar columellar web.
DISCUSSION
One of the cleft lip nasal deformities is the alar-columellar web deformity, in which the excess skin overhangs at the superomedial side of the nostril. Tajima and Maruyama [6] described a reverse-U incision with a suture suspension of the repositioned cleft lower lateral cartilage. Nakajima et al. [7] modified the technique by adding a Z-plasty in the lateral nasal vestibule to correct the alar-columellar web and to prevent tightness of the vestibular area after the rotation of the mucochondrial flap. Cronin and Denkler [16] reported on V-Y plasty of the nasal mucosa left by the advancement of the lateral crus. They proposed that the vestibular lining of the lateral crus remain attached to add circulation and support, especially when scoring of the cartilage is needed. The current author believes that it is important for ample advancement and repositioning of the mucochondrial flap to create a good nasal tip projection. If any nasal vestibular web remains postoperatively, it may place tension on the advanced mucochondrial flap and may even result in the possibility of depression of the repositioned cleft lower lateral cartilage. The current author previously reported excellent results for the correction of unilateral cleft lip nasal deformity using reverse-U incision and V-Y plasty [12]. In addition, Maeda et al. [2] reported using a bilateral reverse-U incision in combination with Cronin's method. Nakajima and Yoshimura [3] used a bilateral reverse-U incision combined with a short banked forked flap in the secondary correction of a bilateral cleft lip nasal deformity.
For an aesthetic appearance of the nose, a well-balanced relationship between the nasal protrusion and the columellar length is very important. The reverse-U incision creates a better nostril contour for Asians. To correct the alar-columellar web deformity, one or two horizontal mattress sutures was placed on the scored area of the reverse-U skin flap, so as to create a concave shape for easy redraping into the concave nasal surface. When the cleft lower lateral cartilage is placed after mobilization, no excessive skin is observed at the nostril. When the cleft lower lateral cartilage is mobilized, the concave external nasal skin becomes embedded into the nasal cavity. However, if the reverse-U flap is excessively rotated superiorly for symmetry, nasal hairs may show. The medial rotation and approximation of the bilateral reverse-U flaps compensates for the insufficient elongation of the columella, as described by Nakajima and Yoshimura [5]. Therefore, mild columellar elongation can be achieved by correcting the alar-columellar web and medially rotating the reverse-U flaps.
After V-Y plasty of a mucochondrial flap, there is dead space between the skin and the repositioned cleft lower lateral cartilage. To avoid this dead space, alar transfixion sutures have been used on the skin and the nasal mucosa [13]. The alar transfixion sutures reattach the repositioned cleft lower lateral cartilage to the nasal skin, thereby giving additional support to the cleft lower lateral cartilage. The most important key suture is located at the superomedial site of the repositioned cleft lower lateral cartilage. The alar transfixion sutures initially cause a dimpling of the skin, which disappears by the second or third week after surgery, without visible scarring. When an adequate and symmetrical nasal tip projection could not be obtained by repositioning the cleft lower lateral cartilage, an onlay-graft of the conchal cartilage was performed to augment the cleft lower lateral cartilage. In this study, the authors placed the cartilage superficial to the cleft lower lateral cartilage and secured it to the medial crura of both lower lateral cartilages.
When the degloved nasal skin is redraped, any tension may affect or distort the projected nasal tip. Columellar lengthening provides structural support for the columella and reduces the tension of the redraped nasal skin. For columellar lengthening, V-Y advancement has been used from the columellar base, nasal floor and alae, central upper lip, or nasal tip [3-5]. However, the current author feels that there are disadvantages of V-Y advancement from the columellar base, including dimpling of the V-Y portion and an unnatural columellar shape. V-Y advancement from the nasal tip or central lip leaves a scar that cannot be hidden. Secondary bilateral banked forked flaps are available for columellar lengthening and nasal tip projection. McComb [8] reported on the unnatural appearance of the nose after columellar lengthening by using the banked forked flap. McComb [8] and Mullikin [9] no longer use the banked forked flap because of the tendency toward abnormally large-shaped nostrils and the inferior drift of the columellar base that has been damaged by scarring. Uchida et al. [4] excised the banked forked flap and reconstructed the columella by mobilizing and rotating the nasal skin, which was combined with bilateral reverse-U flaps.
Composite grafts have been useful for gaining additional columellar length in patients who otherwise have a satisfactory relationship between the lip, nasal tip, and alae [10,11]. Cheon and Park [11] described excellent long-term results of columellar elongation using a conchal composite graft in bilateral secondary cleft lip and nose deformity. They reported the color match was best with preauricular composite tissue.
In this study, a wedge-shaped, full-thickness 0.5 to 1-cm segment of composite tissue was harvested from the helical rim. The defect was closed primarily with less conspicuous scarring. For columellar lengthening, a cartilaginous portion was in contact with the medical crus of the alar cartilage and the skin of the composite tissue was trimmed so as to be fixed to the skin and mucosa of the nose. Accurate wound margin approximation and tension-free suturing are necessary for graft survival in insetting composite grafts. There was no necrosis of the composite graft in this study.
In 22 patients with short columellae treated with composite graft, by combining with reverse-U incision and V-Y plasty of mucoperichodrial flap, alar-columellar web deformity was corrected with simultaneous columellar elongation. Stiffness of a composite graft was similar to the columella. There was no growth disturbance and the elongated columella was well maintained during the 2- to 10-year follow-up period. There was color mismatching in several patients. By way of using of a composite auricular graft for the construction of the columella, the prolabium can be left in its normal position while an improved contour and function of both the lip and the nose is produced [6]. In this study, the average columellar length was significantly improved from 3.7 mm in preoperation to 8.5 mm in postoperation. The average ratio of columellar height to alar base width was 0.18 preoperatively and 0.29 postoperatively.
The current authors created an intranasal retainer using a thermosplint instead of a custom-made design. The size of the retainer depended on the size of the nostril. In addition, all patients used an intranasal retainer, which was centrally hollow to allow for the free passage of air, and was used for 6 to 10 months to prevent scar contracture and to maintain the corrected nasal contour in every patient [12].
In the present study of our series, 4 patients showed fair and poor results with a recurrence of the alar-columellar web and asymmetry of both nostrils. If there was not firm contact between the redraped external nasal skin and the nasal skin, the redraped external nasal skin drooped and the web deformity recurred. Therefore, to avoid this, alar transfixion sutures are recommended on the redraped external nasal skin along with the appliance of an intranasal retainer. Furthermore, alar base advancement or augmentation of the depressed piriform aperture is also important in creating symmetry between nostrils.
In conclusion, the proposed technique of open rhinoplasty with refined reverse-U incision and V-Y plasty or in combination with composite graft was very effective in correcting the bilateral cleft lip nasal deformity by repositioning the cleft lower lateral cartilage to a more normal anatomic position, elongating the columella, and correcting the alar-columellar web deformity.
Notes
This study was presented at the 68th Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 4-7, 2010 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.