Indications, Outcomes, and Complications of Pedicled Propeller Perforator Flaps for Upper Body Defects: A Systematic Review
Article information
Abstract
Background
The aim of this investigation was to systematically review the current literature to provide the best data for indications, outcomes, survival, and complication rates of pedicled propeller perforator flaps for upper body defects.
Methods
A comprehensive literature review for articles published from January 1991 to December 2011 was performed using the PubMed, Medline, and Cochrane Databases. Articles without available full-text, single case reports or papers with excessive missing data were excluded. Papers reporting pedicle-perforator (propeller) flaps used for lower extremity reconstruction were excluded from meta-analysis.
Results
From the initial 1,736 studies our search yielded, 343 studies qualified for the second stage of selection. Of 117 full-text reports screened, 41 studies, met the definitive inclusion and exclusion criteria. Of the selected 41 articles, 26 were case series, original papers or retrospective reviews and were included, whereas 15 were case report papers and therefore were excluded. Two hundred ninety-five propeller flaps were reported to have been used in a total of 283 patients. Indications include repair of trauma-induced injuries, post-trauma revision surgery, cancer resection, chronic infection, pressure sores, and chronic ulcers with a major complication rate (3.3%) comparable to that of free flaps. No specific exclusion criteria for the procedure were presented in the studies reviewed.
Conclusions
Pedicled propeller flaps are a versatile and safe reconstructive option that are easy and quick to raise and that provide unlimited clinical solutions because of the theoretical possibility of harvesting them based on any perforator chosen among those classified in the body.
INTRODUCTION
The propellar flap was introduced with a published series on random subcutaneous pedicle flaps that were elevated and rotated approximately 90 degrees to release scar contractures in the cubital and axillary regions. The knowledge of vessel perforator anatomy, angiosomes, and perforasomes led to the evolution of pedicled perforator flaps, which have simplified the reconstructive options for surgeons in almost every area of the body. After the publication of this pioneering paper, more recent publications have documented the wide clinical application of this technique.
Since pedicled propeller perforator flaps for lower extremity reconstruction have been already analyzed the primary aim of this systematic review was to identify indications, outcomes and survival and complication rates for the use of pedicle propeller perforator flaps in reconstructions of the head and neck, trunk and upper extremities.
METHODS
Search
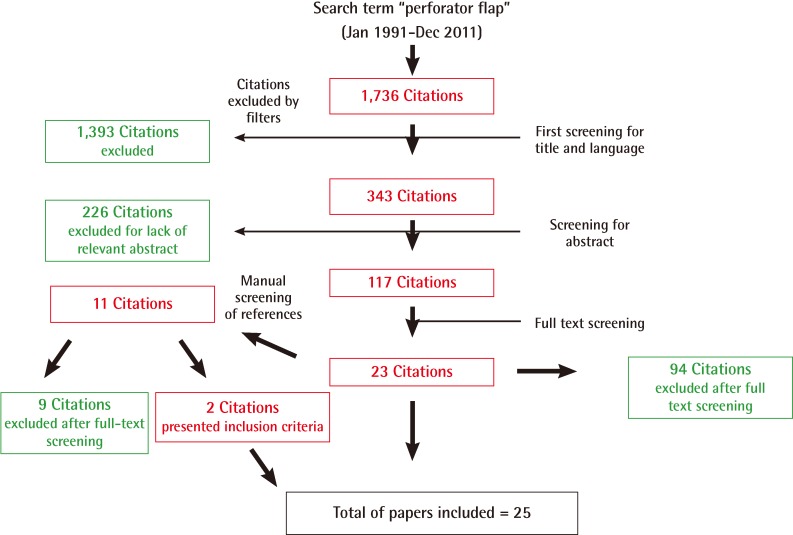
A broad search of the PubMed, Medline, and Cochrane databases was conducted in December of 2011 using the term "perforator flap", and 1,736 original studies published between 1991 and 2011 were identified (Fig. 1). Articles without available full-text, single case reports or papers with excessive missing data were excluded. Papers reporting pedicle-perforator (propeller) flaps used for lower extremity reconstruction were excluded from meta-analysis.
Systematic review search strategy
After the first step of the selection process, the retrieved articles were fully analyzed. Articles reporting a case series in which pedicled propeller perforator flaps were used in human patients for head and neck, trunk and upper extremity reconstruction were included in the final step of the review. If details of the procedure were unclear, the article was excluded. Review papers on this topic that did not present any new cases were excluded.
RESULTS
Of the initial 1,736 studies yielded from our search (Fig. 1), 343 studies qualified for the second stage of selection, and, after the screening of 117 full-text papers, 41 studies met the definitive inclusion criteria. Of the selected 41 articles, 25 were case series, original papers or retrospective reviews [1-25] and were included, whereas 15 were case report papers and therefore were excluded. Among the reports that were included, two hundred eighty-eight propeller flaps have been reported to have been used in a total of 276 patients. The results of the present review are summarized in Table 1.
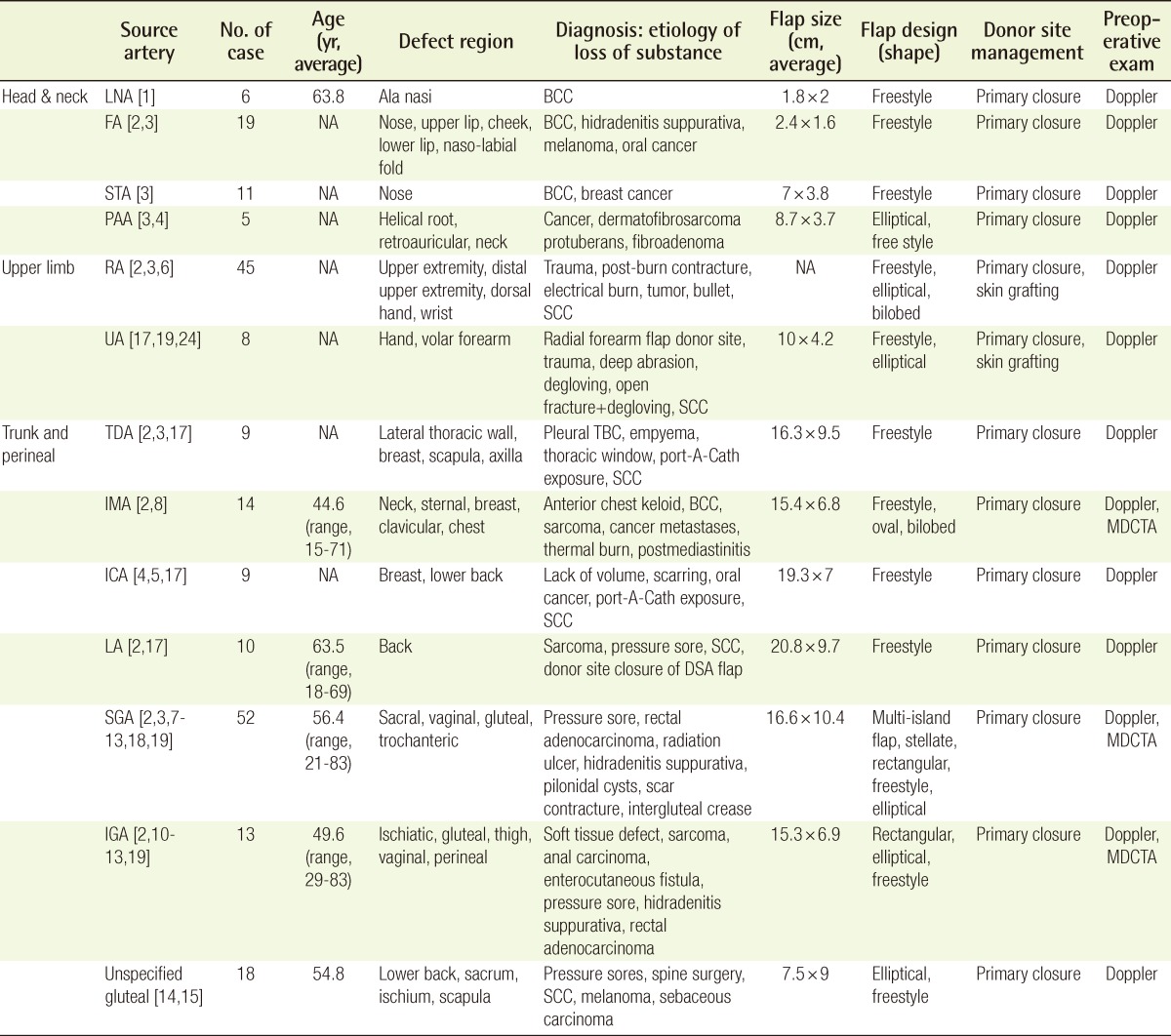
Summary of the most commona) pedicled propeller perforator flaps for upper body defects
Head and neck
A review of the literature revealed a total of 4 articles on the head and neck representing 44 propeller flaps in as many patients [1-4]. The patients had undergone surgery secondary to tumor [4], hidradenitis suppurativa [3] or trauma-induced soft-tissue defects, which affected the following various anatomical sites: the ala [1] and dorsum of the nose [2], naso-labial folds [2], upper and lower lips [3], cheek [3], ear [4], and neck [3]. A total of 19 local propeller flaps within an area adjacent to the defect were harvested from the facial artery perforators [2,3]. In 11 cases [3], the supratrochlear perforator was used as the feeder vessel, and in 6 cases [3], the lateral nasal artery perforators were used as feeder vessels. The posterior auricular artery was the source vessel for 5 flaps [3,4], whereas only 3 cases of transverse cervical artery pedicled propeller flap were described [2,3]. Preoperative Doppler mapping of the perforator vessels was performed in all cases using a handheld device [1-4]. All flaps were dissected in the superfascial/supra-superficial musculoaponeurotic system (SMAS) plane until reaching the vicinity of the marked perforator. The donor site was closed primarily in all patients. Complete flap survival was obtained in all flaps, although 6 patients had minor complications (Table 2). Three cases among the lateral nasal artery propeller series suffered venous congestion that resolved spontaneously [1]. D'Arpa et al. [3] successfully managed a case of arterial insufficiency (supratrochlear artery propeller) using derotation and delayed rerotation of the flap. These authors also managed a case of partial necrosis from venous congestion (facial artery propeller) employing secondary healing.
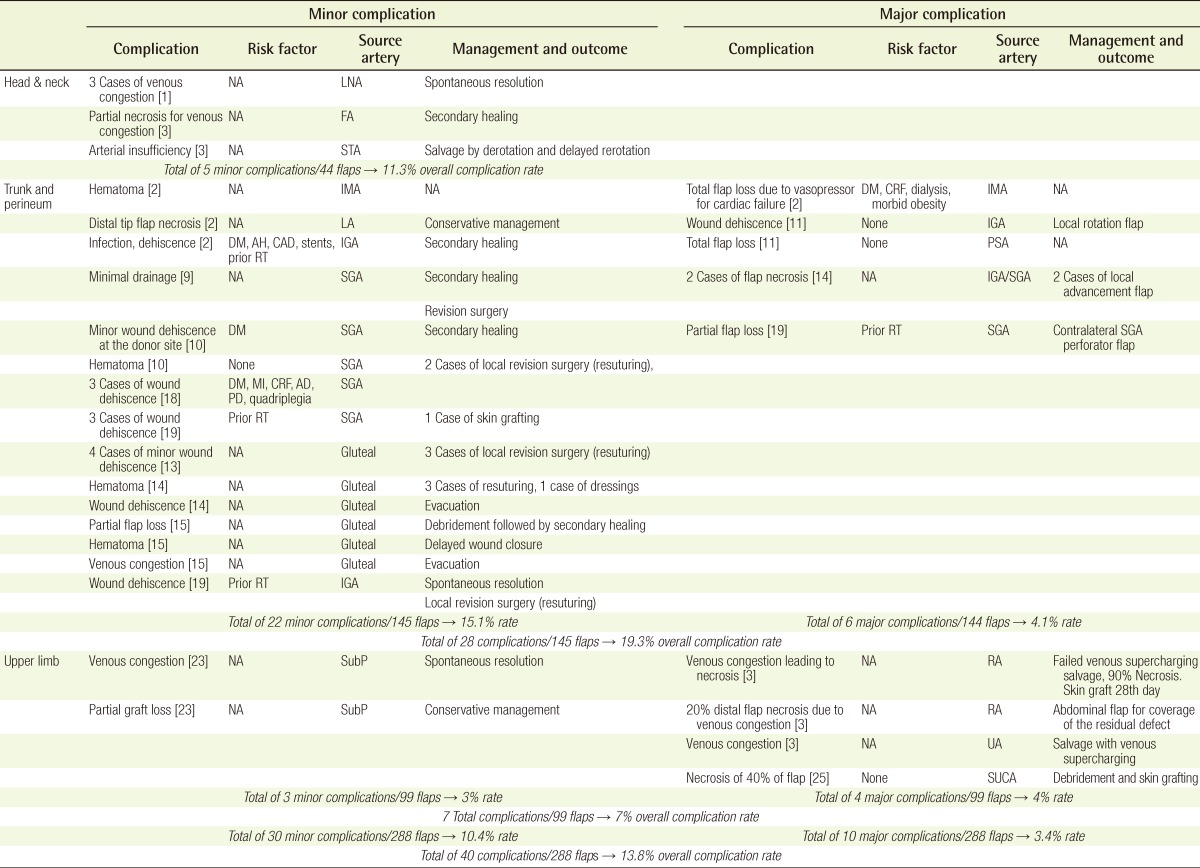
Pedicled propeller perforator flaps for upper body defects. Analysis of complications
Trunk and perineal region
Fifteen articles reporting 145 pedicled propeller flaps in the trunk and perineal region performed in 141 patients were included in this study [2,3,5-17]. Double flaps were used in 4 patients [2,8,19]. The etiologies of the defects included pressure sores [2,3,6,9-11,14,17,18], post-burn sequelae [5,7,8], trauma [6], tumor resection [2,3,8,9,13,15-17], and for sacral radiation ulcer and osteoradionecrosis [19] in almost all patients. Propeller flaps were seldom used for closure of a surgical donor [2], for spine surgery [15] and coverage of Port-A-Cath device exposure [3] and for defects following keloid removal [2], pilonidal cysts [7,8,11] and hidradenitis suppurativa [12].
The gluteal artery perforator propeller flap was the most frequently performed flap [2,3,6-15,18,19], followed by flaps that used the internal mammary [2,8], lumbar [2,17], intercostal arteries [2,3,17] or lateral circumflex femoral artery [18], as the blood supply.
The donor area was primarily closed in all cases. Overall, the flap survival rate was 80.7%, and only 28 patients experienced complications. Four hematomas were drained postoperatively [2,10,14,15]. Wound dehiscence was managed conservatively in 14 cases [2,9,10,13,18,19], and 2 patients required revision with either debridement and skin grafting [14] or local rotation flaps [11]. Distal tip [2] and partial flap necrosis [15,19] occurred in 3 cases and healed uneventfully in 2 patients; in one case a contralateral superior gluteal artery perforator flap was necessary [19]. Four flaps were lost and, in 2 of the cases [14], replaced with local advancement flaps. No information was available regarding the other 2 cases [10]. Among the patients with minor complications, 2 were diabetic [10,18], and 5 were cardiopathic and had received previous radiation therapy at the donor site [2,19]. One of the 2 cardiopathic patients also suffered from diabetes. One partial flap loss due to initial venous congestion required debridement of the flap and coverage with contralateral superior gluteal artery perforator flap because conservative treatment failed [19]. One total flap loss was due to the high dose vasopressors necessary for a patient suffering cardiac insufficiency in the immediate postoperative period [2], and another flap failed in a previously healthy patient [11]. No data regarding comorbidities was available for the remaining patients, who experienced minor and major complications [9,13-15].
Upper limb
Ninety-one upper limb patients were treated with 99 propeller flaps [2,3,7,20-25] for hand, axilla and elbow post-burn contracture [20-23,25] as well as trauma and post-trauma sequelae [2,6,7,23-25], tumor excision [2,3,25], closure of the surgical donor site [3], bursitis [23] and radiodermitis [23]. Eight patients received double flap reconstructions [20]. Many (n=45) of the propeller flaps used the radial artery perforators [2,3,6,23,25] as the axes, and 39 [20-22] were nourished by a subcutaneous random pedicle, using the "central axis flap methods" originally described by Hyakasoku et al. [5]. The source vessels used for the remaining flaps were equally distributed among vessels of the upper limb [2,3,7,22,25]. Flap design and harvesting were performed according to preoperative Doppler evaluations in all cases, except in those studies in which a random subcutaneous pedicle was adopted. In these studies, no mapping of the perforator was provided [20,22]. In a single investigation perforator flaps were planned by mapping the perforators through the use of multirow-detector computed tomography angioscanning [7]. Direct closure of the donor site was achieved in 53 cases [2,7,20-24] and with a skin graft in 4 cases [2,21-24]. In the other 42 cases, these data were not available [3,6,20,25].
A flap suffering from venous congestion was not re-explored because the congestion resolved spontaneously [22]. Necrosis of the distal 40% of the flap (superior ulnar collateral artery perforator flap) in one patient due to flow congestion after primary closure of a flap defect in the arm required debridement and skin grafting. Distal ischemia worsened because of flap thinning just before the inset [24]. Three cases of venous congestion occurred in 2 radial [3,23] and 1 ulnar [3] artery forearm perforator flaps. In a case of necrosis, the residual defect after the debridement (necrosis of 20% of the flap) was covered with an abdominal flap [23]. Two flaps were treated with salvage venous supercharging. The ulnar artery perforator flap survived, and the radial artery perforator flap failed, more than likely as a result of delayed re-exploration. The latter was debrided and grafted 1 month later postoperatively [3]. The comorbidities of the patients who experienced minor and major complications were not stated within the papers [3,23,24].
DISCUSSION
With the present investigation we have systematically reviewed the current literature on this topic, providing additional insight on pedicled propeller flap safety and feasibility for upper body defect reconstructions with indications including defects following trauma and post-trauma revision surgery, cancer resection, chronic infection, pressure sores, and chronic ulcers (Tables 1, 2). Within the literature analyzed, 288 propeller flaps were used in a total of 276 patients with an overall complication rate of 13.8% (Table 2) [1-25]. Although this data should raise further concerns regarding the safety of propeller flaps, the major complication rate (3.4%) is comparable to that of other series of free flaps.
There are contrasting opinions regarding the use of the supraor subfascial plane for dissection. Although the chosen dissection plane is usually subfascial, there is no difference in the survival rate between fasciocutaneous [2,9-11,15,23,24] and adipocutaneous [1-3,6,17,23,25] propeller flaps (in one third of the articles reviewed, these data were not available [5,7,8,12,13,16,20-22]). Although the fascia is not necessary to augment the blood supply, in almost all papers, the subfascial approach is suggested for surgeons who have little experience in perforator surgery because this technique allows for efficient flap harvest and a clear visualization and isolation of the pedicle [2,3,25]. Although, in general, subfascial dissection is technically easier, suprafascial dissection leaves a less consistent donor site defect and makes flap dissection simpler at the sites where the muscular septa join the muscular fascia [2,3,25].
The location of the best perforator closest to the defect has been detected preoperatively with a handheld Doppler in almost all cases. In a few papers either multidetector-row computed tomography angiography (MDCTA) [7,8,23] or computed tomography angiography (CTA) [13,16] were adopted. From the review the superiority of MDCTA over the other less invasive imaging techniques should be presumed even if comparative studies are required, because it allows for determining a more precise location of the perforator and its subcutaneous course through 3D reconstruction imaging [7,9,23]. Anyway, using a handheld Doppler scanner to locate perforators followed by a quite generous incision to verify and choose the perforator during surgical exploration has been preferred by almost all authors. In this way different potentially useful perforators were made visible and the best one for the size and location was chosen. This procedure was considered less time-consuming, less expensive, repeatable and, with increased ability to perform propeller flaps, safe [1-6,9-19,21-25]. In no paper was Doppler imaging indicated to be the cause of inaccurate preoperative assessment (absence of perforator).
Propeller flap surgery should follow these principles. Flaps should be based on perforators as close to the midline or a fixed point (shoulder, elbow, and wrist in the upper extremity) as possible and be marked along the axis of the main source vessel. The safest orientation of the main axis of the flaps is transverse (perpendicular to midline) for the trunk and longitudinal for the upper extremity [2,3]. This positioning allows the vascular axis of flow between the perforator vascular territories to follow the direction of linking vessels [2,3]. Consequently, it is of great significance to consider the axiality of the blood flow when the skin paddle flap is designed because the perforasomes from the same source artery are filled preferentially over adjacent vascular territories from other source arteries [7]. Due to highly variable anatomy, no rule regarding the maximal number of perforasomes to be included in a single-perforator flap has been validated [2,3]. Furthermore, it has been assumed that hyperperfusion in a single perforator flap leads to increased filling pressure, triggering the recruitment of neighboring perforasome territories. However, it is still unknown whether a limitation in the size of the perforator-based propeller flap should exist. Thus, questions regarding the correlation between the size of a perforator, its perfusion, and the largest volume of tissue that it can safely sustain remain unanswered and no precise guidelines on flap size can be suggested. In our review, two of the largest flaps nourished by a single 1-mm perforator measured 25×30 cm (750 cm2, superior gluteal artery perforator) and were successfully used to resurface a 15×20 cm sacral defect [9], respectively. Thus, some authors have suggested that the real limitation of the flap size nourished by a single perforator should most likely be its design to allow donor site closure, rather than concerns about vascularity [3]. The empiric principle of the length-to-width ratio used for fasciocutaneous flaps needs to be revised and should not be applied to achieve a mathematic rule of safety for perfusion of freestyle pedicled-propeller flaps [3]. The eccentric location of the perforator defines the edge of the two blades of the propeller, splitting it into two skin islands, each with its own ratio. That is, a flap measuring 22×4 cm should not be considered as having a 5.5:1 ratio, but a perforator entering the flap at a point 8 cm from the tip splits the flap in two 8×4 cm and 14×4 cm minor skin island flaps with 2:1 and 3.5:1 ratios, respectively. To enlarge safely the original size of the perforator-based propeller, the location of a dominant perforator for supercharging in the distal part of the flap is confirmed preoperatively [8]. During flap elevation the perforator and its concomitant vein is left attached at the distal part of the extended flap, then they are anastomosed with the recipient vessels after the flap inset in the recipient site [8]. Venous supercharging alone may be adopted when venous insufficiency occurs by anastomosing a vein of the flap or a vein of a second perforator to a vein of the recipient site [2,3].
Pedicled propeller perforator flaps have widened the array of options for reconstructive surgeons. Because of their relatively recent introduction, skepticism has overshadowed their safety in clinical practice. This review showed that the major complication rate (3.4%) is comparable to those of free flaps that are widely considered safe. The ability to employ any perforator found close to the defect, which is capitalized upon with the propeller flap technique, grants the surgeon the freedom to customize skin islands, resurface defects with importation of undamaged tissue for easy closure without tension, and create pleasant cosmetic outcomes without the sacrifice of any recipient vessels and with the preservation of muscle function.
Notes
No potential conflict of interest relevant to this article was reported.