Evidence-Based Analysis of Lymph Node Transfer in Postmastectomy Upper Extremity Lymphedema
Article information
Upper extremity lymphedema is one of the most important sequelae of mastectomy and affects an estimated 16 to 39% of breast cancer patients [1]. Few surgical options for lymphedema have achieved satisfactory long-term results. Amongst previously described methods, the microvascular lymph node transfer (LNT) is the most promising and appears to provide significant improvement, especially in early stage lymphedema.
We evaluated the existing literature, looking at the influence of LNT on postmastectomy upper extremity lymphedema through a systematic review.
We searched the PubMed database for English articles published from January of 1990 to March of 2012. Our keywords included "postmastectomy lymphedema", "upper extremity lymphedema", "lymph node transfer", and "vascularized lymph node". This search was supplemented by a review of reference lists of potentially eligible studies. We excluded experimental studies, case reports, and studies in which the results were not separated for the upper and lower limbs. Two reviewers independently extracted data in two steps: titles and abstracts, and then full-text articles. Through our electronic and reference search, we identified 5 clinical studies (Table 1) [1-5]. All of the studies were case series (level IV evidence).
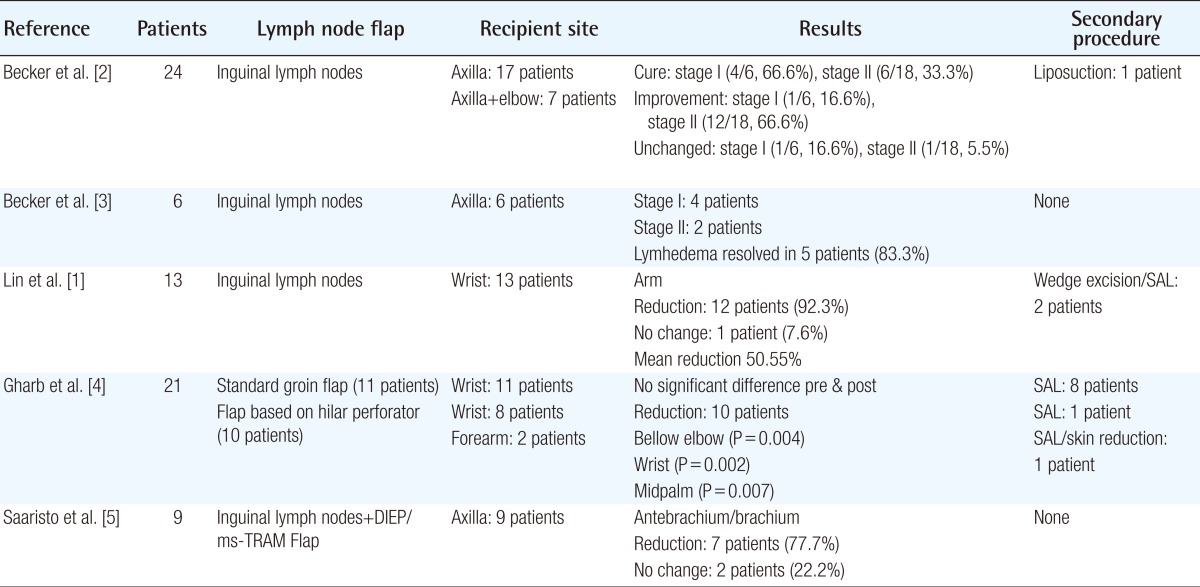
The five clinical studies on lymph node transfer in postmastectomy upper extremity lymphedema
In total, 73 patients received LNT for postmastectomy upper extremity lymphedema. The recipient site was the wrist in 32 patients (43.8%), the axilla in 32 patients (43.8%), the forearm in 2 patients (2.7%), and 7 patients (9.5%) received two LNTs (axilla and elbow).
Lin et al. [1] used a groin flap containing lymph nodes based on the superficial circumflex iliac vessels and the anastomoses were performed to the superficial radial artery and cephalic vein. Becker et al. [2,3] used a similar groin flap but as recipient vessels, used the circumflex scapula vessels. Gharb et al. [4] described a modification of the classic groin lymph node flap. The authors used the superficial branch of the superficial circumflex iliac artery as the dominant vessel responsible for the vascularization of the lymph nodes. The wrist was used as a recipient site, with the anastomosis to the radial artery end-to-side, and the concomitant veins of the radial artery end-to-end. Saaristo et al. [5] combined the breast reconstruction using abdominal flaps with the transfer of vascularized inguinal lymph nodes based on the superficial circumflex iliac vessels or the superficial inferior epigastric vessels, and the anastomoses were performed from the deep inferior epigastric vessels end-to-end to the thoracodorsal vessels.
According to the research, there is no consensus on the staging of lymphedema. Only three studies [2-4] have reported precise preoperative staging systems; however, each study used different criteria. Fifty-seven of 73 patients (78%) had postoperative improvement of the affected limb. In every study, a different postoperative evaluation method was used, and the relationship between the lymph node recipient site (axilla, elbow, or wrist) and the anatomical site with the maximum improvement was not clearly reported.
Becker et al. [2] reported that from the 18 patients, the upper limb perimeter returned to normal in 10 cases, remained unchanged in 2 cases, and decreased by more than 50% of its value in 6 patients and less than 50% of its value in 6 other patients. Two years later, Becker et al. [3] evaluated the influence of LNT in postmastectomy neuropathic pain in 6 patients. All of the patients had relief of the symptoms and in 5 patients the lymphedema resolved. Gharb et al. [4] compared the classic groin lymph node flap with a groin flap based on hilar perforators and reported that differences between the preoperative and postoperative measurements were statistically significant only in the perforator-based group at the levels below the elbow, wrist, and midpalm. Saaristo et al. [5] achieved reduction of the affected limb in 7 of 9 patients.
Even though it is implied that at early stage lymphedema, the LNT has better results, the influence of LNT at each stage of lymphedema is not clear. In addition, 17.8% of the patients required an additional procedure (suction assisted lipectomy [SAL] or skin excision) due to lack of sufficient improvement after LNT.
According to existing clinical studies, LNT is able to alleviate postmastectomy upper extremity lymphedema. However, the improvement is variable and no conclusions have been drawn regarding which technique, group of donor lymph nodes, or recipient site can ensure the maximum reduction of the affected limb.
More clinical studies are needed, and a consensus about the staging system of lymphedema and the evaluation methods for postoperative results should be established to enable drawing more certain conclusions.
Notes
No potential conflict of interest relevant to this article was reported.