Abdominoplasty Access for Desmoid Tumor Resection in the Rectus Abdominis Muscle
Article information
With great interest we read the article "desmoid tumor of the rectus abdominis muscle in a postpartum patient" by Choi et al. [1]. In their article, the authors describe a case of a 36-year-old woman who presented with a painless mass in the right rectus abdominis muscle after delivery of two children, the latter three years before presentation. The authors resected the desmoid tumor with parts of the surrounding muscle through a small skin incision, localized directly over the tumor mass. Besides the aforementioned direct approach to the tumor mass and the usage of preexisting scars, other methods have also been described [2,3]. We would like to share our surgical approach in a similar case in our department that we think is superior for several reasons.
A 26-year-old female patient presented with a painless mass on the right abdominal region next to the umbilicus, which she had noticed 2 weeks earlier (Fig. 1). Similar to the case presented by Choi et al. [1], our patient did not have any family history of desmoid tumors, familial adenomatous polyposis syndrome, or Gardener syndrome. She was a non-smoker, did not drink alcohol, and had no history of trauma. She had given birth to one child by cesarean section 2 years earlier. Ultrasound revealed an undefined vascularized tumor in the right rectus abdominis muscle. A T1-weighted magnetic resonance image (MRI) revealed an 8 cm×3.2 cm×1.8 cm tumor mass in the right rectus abdominis muscle with high contrast medium enhancement without signs of infiltration of the surrounding fatty tissue or intra-abdominal structures, strongly resembling a desmoid tumor (Fig. 2). After punch biopsy, the histological examination revealed a strong suspicion of a desmoid tumor. After having discussed this case in our interdisciplinary tumor board, the decision for wide resection was made. Exposure of the anterior layer of the rectus sheath was performed via the preexisting scar of the cesarean section through an abdominoplasty approach (Fig. 3). Abdominoplasty was basically performed as described by Pitanguy et al. [4]. A solid mass was palpable in the right rectus abdominis muscle without macroscopic signs of tumor invasion of the rectus sheath. A wide local excision with a 3 cm circumferential resection margin of healthy tissue was performed. The abdominal wall was reconstructed with nonabsorbable polypropylene surgical mesh (Surgipro, Covidien, Mansfield, MA, USA) and the defect closed in layers (Fig. 4). Histological examination yielded clear resection margins with a minimum of 32 mm on circumferential measurement after wide excision. After 6 months the patient showed no signs of relapse of the desmoid tumor and an excellent aesthetic outcome (Fig. 5). Follow-up MRI was performed 6 months postoperatively. Regular long-term follow-up visits are scheduled as desmoid tumors show aggressive clinical behavior such as repeated local recurrence.

The patient presented with an 8 cm×3.2 cm×1.8 cm painless mass on the right abdominal region next to the umbilicus.
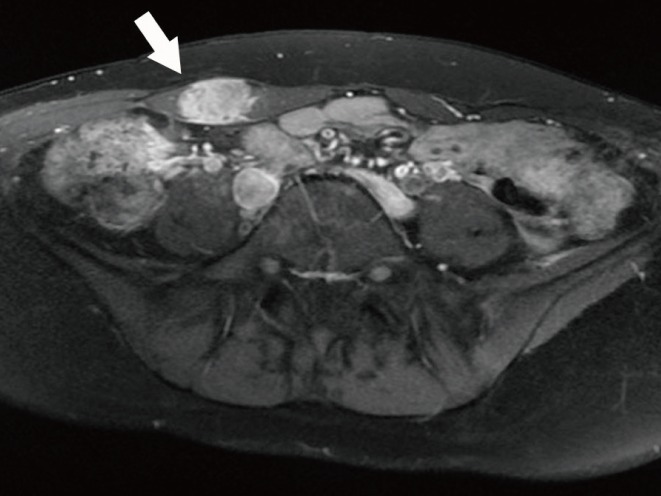
Preoperative magnetic resonance imaging findings of a hypodense mass in the right rectus abdominis muscle (white arrow).

Intraoperative photo of the intramuscular tumor with a 3 cm circumferential resection margin of healthy tissue in the right rectus muscle.
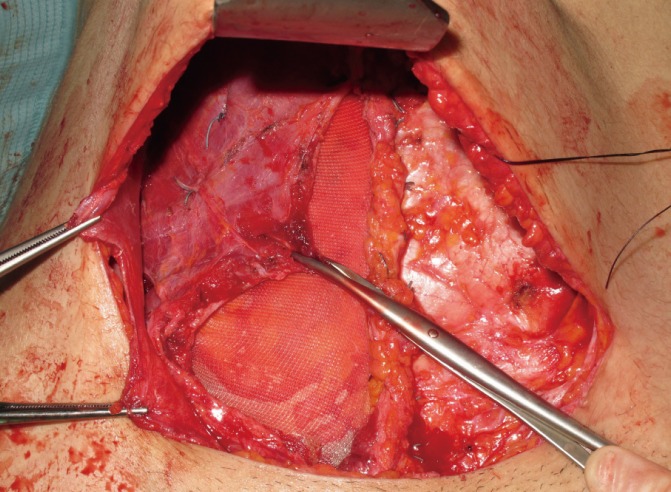
The abdominal wall was reconstructed with nonabsorbable polypropylene surgical mesh and the defect closed in layers.

Final appearance of the abdominal region after 6 months.
Abdominoplasty has been described before for aesthetically pleasing results for defect coverage after wide resection of abdominal dermatofibrosarcoma protuberans [5]. Similarly our abdominoplasty approach for resection of desmoid tumors in this location allows for a naturally appearing abdomen with very little to no donor site morbidity and almost invisible scaring, which can easily be hidden by the patient's underwear. The cosmetic result achieved with this surgical technique is excellent (Fig. 5) and in our opinion is far superior to the aforementioned described techniques, especially in postpartum patients who frequently benefit from a full abdominoplasty. In addition, coverage of wide resection defects is easily achievable.
The advantages of the abdominoplasty approach for desmoid tumor resection and abdominal wall repair are improved and unparalleled cosmetic outcome, and minimal donor site morbidity achieved by a single-stage procedure. To our knowledge, this is the first report of an abdominoplasty approach for desmoid tumor resection and abdominal wall repair in the literature. In conclusion, we recommend this technique for its technical ease and superior outcome provided that there is no evidence of infiltration of adjacent tissue. We would like to emphasize that our abdominoplasty approach is by no means a technique for each and every case. Of course, some cases will yield functional deficits, for example, if extensive resections have to be carried out. However, in selected cases, this technique is a worthwhile alternative to be considered. Clearly, in each case, tumor- and patient-specific factors such as localization, size, anatomic structures affected, and estimated resection margins have to be taken into account, and therefore deliberate consideration has to be given to other reconstructive methods available as well.
Notes
No potential conflict of interest relevant to this article was reported.