Hidden Sentinel Node in Cutaneous Melanoma
Article information
Sentinel lymph node (SLN) biopsy is a well-established staging method for melanomas. Several techniques have been described to identify the first lymph node receiving lymphatic flow from the primary tumor. Injection of 99mTc-nanocolloid into the tumor bed followed by lymphoscintigraphy provides a road map for the surgeon. However, in a variable percentage of cases, the sentinel node may remain undiscovered during this procedure [1]. This problem is well-known with regard to the identification of lymph nodes in the head and neck, where the complex anatomy as well as the presence of vital structures renders lymphatic mapping a challenging procedure [2].
Hence, we would like to share our experience in this field by describing the case of a 40-year-old woman who was referred to our department for a 1.33-mm-thick melanoma of the upper external quadrant of the left breast (Fig. 1). Previous surgical excision had been followed by histopathologic analysis reporting an infiltrating cutaneous melanoma with vertical growth and a mitotic index=2, and without ulceration.
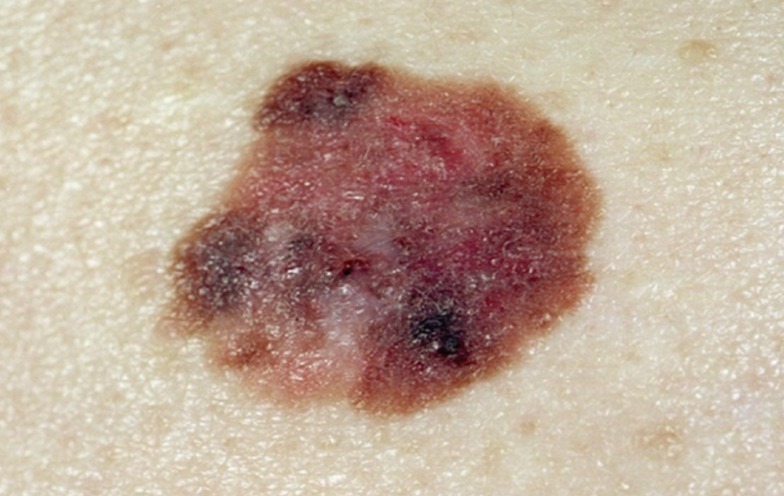
Melanoma of the upper external quadrant of the left breast.
As a consequence, the patient underwent lymphoscintigraphy (Fig. 2). Planar imaging of the thorax was performed 10 minutes, 30 minutes, and 2 hours and 4 hours after the injection of the radiopharmaceutical. No hot spot could be identified as a sentinel lymph node. Hence, lymphoscintigraphy was postponed for two weeks but, again, neither lymphatic drainage nor a sentinel lymph node was shown. One day later, intraoperatively, a γ-ray detection probe (Navigator, USSC, Norwalk, CT, USA) was used through the intact skin to check the axilla. No radioactivity was found and, in consultation with our institution's oncologists, axillary lymphadenectomy was planned. Widening of the margins was performed, and the hand-held gamma probe was subsequently inserted into the resulting defect (Fig. 3). Radioactivity was found on the deep upper portion of the defect. An accurate dissection, guided by a gamma probe, was performed, and one radioactive node was removed. After removal of the sentinel node, the wound showed no further radioactivity. As a consequence, lymphadenectomy was not performed. Histological analysis of the sentinel node showed the presence of metastatic cells.
Lymphoscintigraphy of the patient with an image at 10 minutes after the injection of the radiopharmaceutical. No hot spot could be identified as a sentinel lymph node.

Preoperative image of the patient undergoing widening of the margins of the previous melanoma excision. Left oblique view of the breast with the scar of the previous melanoma excision.
Sentinel node biopsy was first introduced in melanoma patients in 1992 [1]. Since this initial experience, several techniques have been described to identify the first node receiving lymphatic flow from the primary tumor. Preoperative mapping by mean of lymphoscintigraphy has become of paramount importance in melanoma patients due to the unpredictability of lymphatic drainage patterns [3]. However, there are some reports in the literature describing its failure in identifying the SLN. Jansen and colleagues showed that the predicted number of sentinel nodes detected with lymphoscintigraphy was accurate in only 81% of lymph node fields and that its limited discriminating power was the most frequent reason for discrepancies with surgical findings [1]. Hidden sentinel nodes have also been reported in breast cancer patients. Several techniques have been suggested to address this problem, such as delayed imaging, re-injection of the radiopharmaceutical, post-injection massage, injection of saline around the tumor, and hybrid single-photon emission computed tomography/computed tomography (SPECT/CT) scan.
In our patient, no sentinel node was shown by lymphoscintigraphy. Two reasons were hypothesized to be responsible for this finding: disruption of the lymphatic drainage induced by surgical excision or concealment of the axillary sentinel node behind the injected radioactivity. Intraoperatively, the latter proved to be true, thus overcoming the need for primary lymphadenectomy.
Lymphoscintigraphy is an important guide for sentinel node biopsy, but it may sometimes fail to provide an adequate road map for the surgeon, as in our patient. In such cases, multi-directional scintigraphic views must be considered, in order to detect hot nodes concealed by the injection site, as described for axillary nodes in breast cancer of the upper lateral quadrant [4]. The intraoperative use of blue dye and/or a gamma probe is of paramount importance to compensate for the limitations of scintigraphy, thus allowing the surgeon to perform an oncologically adequate procedure and to spare the patient primary or wrong-site lymphadenectomy.
However, the use of blue dye may produce adverse effects, such as urticaria, hypotension, and bronchospasm, and may have marginal benefits, as described by Lingam et al. [5].
As a consequence, intraoperative gamma probing remains a mainstay in cases of hidden nodes or false-negative scintigraphic findings.
Notes
No potential conflict of interest relevant to this article was reported.