Breast Reconstruction in a Previously Explanted Patient: An Interesting Anatomical Anomaly
Article information
Breast prostheses have been available since the 1950s, serving the purpose of improving the breast contour in breast reconstruction and augmentation. Explantation of breast implants may be required for a variety of reasons including capsular contracture, damage or change in size and shape of the implant, or fear of the potential adverse effects of the implants on health [1]. The complications and effects of explantation are well recorded but a consequential alteration of the pectoralis major anatomy has not yet been presented in the literature.
We present an explantation-induced anatomical anomaly of the pectoralis major identified in a patient undergoing ipsilateral mastectomy followed by tissue expander reconstruction. The salient features of this case and the operative considerations served as the foundation for the discussion.
A 75-year-old Caucasian female presented with an upper quadrant mass in her right breast. This was confirmed on examination and was associated with ipsilateral skin dimpling, bilateral inframammary fold scars, and no axillary lymphadenopathy. Her surgical history was significant for bilateral subglandular breast augmentation with gel-filled silicone implants in 1977. Bilateral explantation and capsulectomy were then performed in 1994 via the previous inframammary scars because of leakage of both silicone implants and capsular contracture. Dissection was found to be particularly challenging because of the considerable amount of calcification and scarring on the capsule, surrounding breast tissue, and underlying pectoralis muscle.
Magnetic resonance imaging (MRI) visualized locally advanced multifocal cancer in the right breast. The largest tumor was 3.5 cm in diameter. A biopsy confirmed a well-differentiated infiltrating ductal carcinoma (estrogen receptor/progesterone receptor positive, and Ki-67 was 5%). She underwent a 2-year course of neoadjuvant hormonal therapy (anastrozole) with a good response.
In January 2013 the patient underwent ipsilateral total mastectomy, positive sentinel lymph node biopsy, and subsequent level 1-2 axillary dissection and tissue expander reconstruction. The skin flaps were elevated, the right breast was removed en bloc, and the pectoralis major was exposed. No capsular tissue was present, but interestingly, the muscle found was entirely released from the 6th rib and retracted superiorly and medially (Fig. 1). The only attachment was to the sternal border. This anomaly caused exposure of 60% of the tissue expander (Allergan 133 MB 13) when located in the pocket under the muscle, making the use of acellular dermal matrix (ADM) essential. Following pectoralis major mobilization and the correct location of the tissue expander, a 16 cm×8 cm sheet of ADM was sutured along the inframammary fold and the free edge of the pectoralis major. 180 mL of sterile saline were then placed in the tissue expander. The wounds were then closed, and 2 suction drains were left in situ.
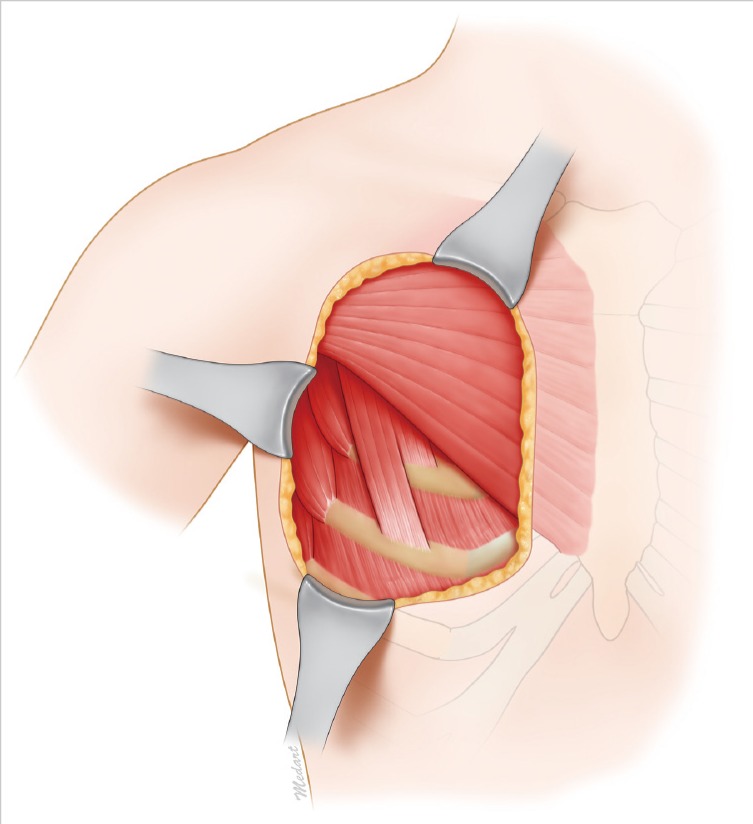
Shows the pectoralis major anomaly visualized during surgery. The muscle found was entirely released from the sixth rib and retracted superiorly and medially. The only attachment was to the sternal border. Illustration adapted from Dr. F. M. Egro's illustration.
This case presents a very unusual anatomical anomaly not described elsewhere in the literature. The significance is not purely academic, in that the anomaly has important implications for intraoperative execution and adequate preoperative planning.
The pectoralis major muscle has 2 heads: clavicular and sternocostal. The former originates from the anterior surface of the medial half of the clavicle, while the latter originates from the anterior surface of the sternum, the six superior costal cartilages, and the aponeurosis of the external oblique. Both heads insert into the lateral lip of the bicipital groove of the humerus. It was therefore a surprise to find the muscle completely displaced superiorly and medially.
Anomalies to the pectoralis major muscle have been described. The best-known congenital deformity is Poland's syndrome, where malformation of the chest causes the pectoralis major on one side of the body to be absent [2]. Other rarer anomalies include an accessory head originating in the abdominal wall [3], the existence of only the pars clavicularis [4], or only the clavicular and part of the sternocostal portion [5]. However, in these cases, the pectoralis minor muscle was found to be defective, which was not the case in our patient. Furthermore, given the history of breast augmentation, explantation, and capsulectomy, we hypothesize that this was an acquired deformity.
This type of deformity might be expected in patients who previously underwent submuscular (and not subglandular) breast augmentation, because the pectoralis major is normally separated at its caudal and medial point of attachment, that is, along the rib from the intermediate area medially in the direction of the sternum. Explantation of the breast implant is performed for a variety of reasons, but fear of the possible harmful consequences is the most common one. Normally, the incision and dissection follow the original site. A capsulectomy is routinely performed followed by careful hemostasis and irrigation of the pocket [1]. The complications of breast implant explantation have been recorded, and these include: seroma, bleeding, infection, ptosis, asymmetry and deformity, loss of nipple/areola sensation, and emotional impact [1]. However, this unique intraoperative finding has not yet been described. Furthermore, the challenges that one must consider during reconstruction of a previously explanted breast have not yet been discussed.
The senior author elected preoperatively to use ADM to cover the tissue expander without knowing that it would become essential. By this, we mean that without its use, the tissue expander could not have been safely secured in the subpectoral pocket because of the minimal coverage of the tissue expander by the pectoralis major muscle. At the time, the only alternative would have been coverage with an autologous flap such as that of the latissumus dorsi. Had we known about this anomaly, preoperative planning would have included imaging (MRI) and appropriate consent. The significance of this in clinical practice is twofold: 1) improvement of surgical and aesthetic outcomes.had we not had ADM onsite (which is the case in many US and non-US hospitals), we would have had to resort to a much more complicated procedure, with greater morbidity and more scarring; and 2) medico-legal issues since the patient might not have provided adequate consent for an autologous flap.
Given our findings, the following algorithm (Fig. 2) might be useful when considering breast reconstruction (with a tissue expander) in a patient who has undergone previous explantation.
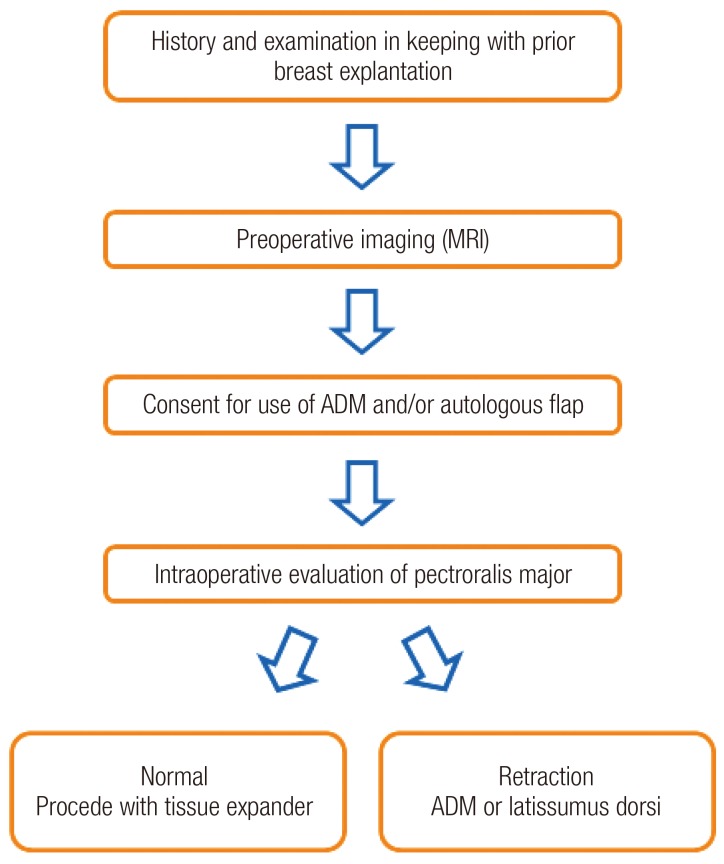
Shows an algorithm to be used when considering tissue expansion reconstruction in a patient who has undergone previous implant explantation. MRI, magnetic resonance imaging; ADM, acellular dermal matrix.
This article presents an important anatomical anomaly that requires consideration in all patients requiring tissue expansion reconstruction who have undergone previous implant explantation. The importance lies in the need for adequate preoperative evaluation of the patient and the adjustments that might be required intraoperatively for an optimal surgical outcome.
Notes
No potential conflict of interest relevant to this article was reported.