Penoscrotal Extramammary Paget's Disease with Multiple Lymph Node Metastasis
Article information
Extramammary Paget's disease (EMPD) is an uncommon intraepithelial adenocarcinoma. EMPD in the penis and scrotum, first described in 1888, is extremely rare [1]. EMPD is a rare skin disease that is limited to the epidermis, but has the potential to invade the dermis and metastasize. If dermal invasion has occurred, the rate of lymph node or distant metastasis will increase [2]. The rate of lymph node metastasis is reported to be 26% in patients with invasive primary lesions [3]. EMPD might be associated with an increased risk of underlying internal malignancy of the lower gastrointestinal or genitourinary tract. We describe a case of penoscrotal extramammary Paget's disease with multiple lymph node metastasis.
A 69-year-old man was referred to us with a one-year history of a painless erythematous skin rash on the penis and scrotum (Fig. 1). He first visited a local clinic and was treated with topical agents. Despite conventional treatment, the lesion extended to the scrotum and penis. The patient initially underwent a punch biopsy and the pathology report came back as EMPD. On physical examination, there was a 2-cm round, firm mass in the left inguinal area. A computed tomography (CT) scan of the abdomen revealed a 2.1-cm round peripheral rim-enhancing lymph node (LN) in the left inguinal area and a 2.8-cm enlarged ovoid lymph node in the right inguinal area (Fig. 2). Ultrasound-guided biopsy of the localized mass in the left inguinal area confirmed the diagnosis of metastatic carcinoma.

Preoperative view: a 69-year-old male patient with penoscrotal extramammary Paget's disease.
A computed tomography scan of the abdomen revealed bilateral inguinal lymph node metastasis. The white arrow indicates a 2.1-cm round peripheral rim-enhancing lymph node in the left inguinal area.
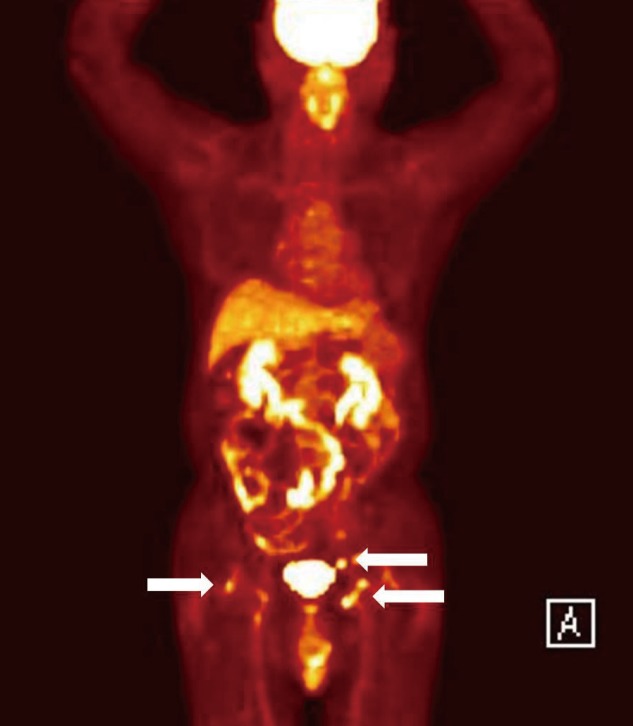
Before wide excision of the scrotal and penile lesion, mapping biopsies were performed to determine the exact margins of the lesion. However, during the preoperative period, the mass of the right inguinal area increased from 2.8 to 3.58 cm. Therefore, the patient was admitted to the department of oncology and had an extensive cancer work-up. The tumor markers were within normal range: alpha-fetoprotein 1.5 ng/mL (normal range, 0-20 ng/mL), carcinoembryonic antigen 2.6 ng/mL (normal range, 0-5 ng/mL), and prostate-specific antigen 0.712 ng/mL (normal range, 0-3 ng/mL). Routine colonoscopy and esophagogastroduodenoscopy were performed to check for internal malignancy of the lower gastrointestinal track. However, there was no evidence of an underlying internal malignancy. A whole-body positron emission tomography (PET)/CT scan revealed metastatic lymphadenopathy on both inguinal areas and the left external iliac space. No other abnormal hypermetabolic lesion was found (Fig. 3).

A full body positron emission tomography computed tomography scan showed metastatic lymphadenopathy in both inguinal areas and the left external iliac space (white arrows).
After the full cancer work-up, the patient underwent wide local excision with both inguinal and left external iliac lymphadenectomy. We performed surgical wide excision of a 16.5 cm×8.5 cm lesion of the scrotum and penis. The skin defect was covered with a scrotal flap and split-thickness skin graft for the penile shaft.
The pathologic findings with immunohistochemical staining revealed extramammary Paget's disease (Fig. 4), measuring 7 cm×4.2 cm. Moreover, a 1.5 cm×1 cm dermal invasion lesion of the penis and scrotum was seen (Fig. 5).
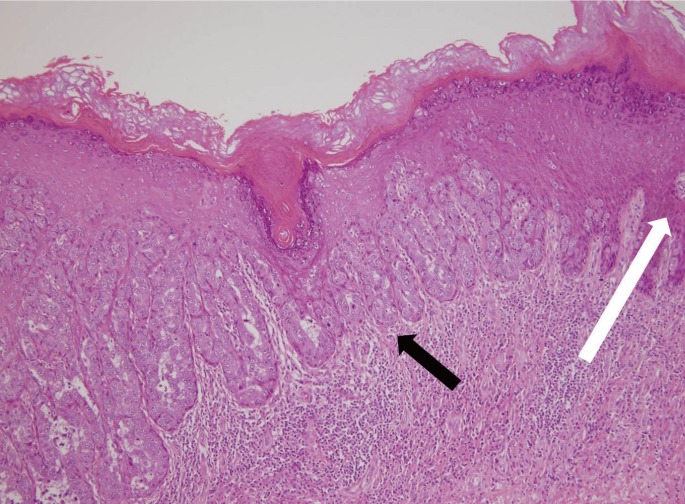
Histological findings. The black arrow indicates Paget cells with atypical round nuclei with abundant pale granular cytoplasm. The white arrow indicates normal cell lining (H&E, ×100).
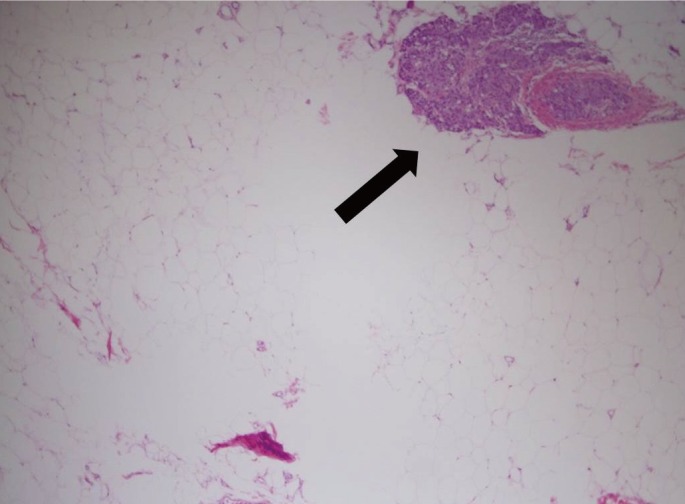
Histological findings. The black arrow indicates a tumor cell nest in the subcutaneous layer (H&E, ×20).
All of the surgical safety margins were clear. In this report, our data showed that 17 of 20 lymph nodes showed metastasis. The lymph node metastasis was expressed in 75% (3/4) in the right inguinal, 85.7% (6/7) in the left inguinal, 100% (6/6) in the left external iliac, and 66.6% (2/3) in the peri-iliac vessel.
An abdomino-pelvic CT scan was performed 1 month postoperatively. Based on the CT scan data, a 1.8 cm×2.5 cm lymphocele was found in the left external iliac and inguinal region. However, there was no evidence of metastasis in the abdomen or pelvis. The patient received 45 Gy/25 Fx postoperative radiotherapy. He was followed up in the outpatient department for 6 months without any evidence of recurrence or other complications.
EMPD is a rare, slow-growing intraepithelial lesion with well-defined moist erythematous or white plaques. Complete surgical excision is the treatment of choice for EMPD. Mohs micrographic surgery or mapping biopsy is useful for determining the normal skin margin for wide excision. Non-surgical treatments, such as radiation therapy, topical chemotherapy with imiquimod, and photodynamic therapy with topical aminolevulinic acid are effective in inoperable patients. Only radiation therapy can be applied for deep lesions such as lymph node metastasis. Several authors have reported on EMPD patients treated with radiation therapy at total doses of 30 to 54 Gy in 3 to 25 fractions. However, the optimal radiation dose for treatment of a metastatic lymph node is controversial [4].
EMPD rarely invades the dermis or spreads to the local inguinal lymph nodes or remote sites; only a few such cases have been reported. Chan et al. [2] reported that dermal invasion was found in 18.8% on histological examination after wide excision. Regional lymph node metastasis was found in 14.5%, and there was a statistically significant relationship between dermal invasion and regional lymph node metastasis. In cases of primary invasive tumor without clinical lymph node metastasis, elective lymph node dissection has been recommended [3]. Our case showed a focal dermal invasion in the primary lesion with bilateral inguinal and left external iliac LN metastasis. The standard treatment for advanced EMPD with distant metastasis is controversial. We performed successful wide excision, obtaining clear margins, and multiple lymphadenectomy. We applied additional radiation therapy because most of the pathologic findings of the lymph nodes were positive. There have been some reports about the clinicopathology and prognosis of metastatic EMPD [5]. However, they have not been well established, so further clinical follow-up is needed.
Notes
No potential conflict of interest relevant to this article was reported.