K-Wire Breakage During Metalware Removal Due to a Defective K-Wire Shaft
Article information
Since its introduction in 1909 by Martin Kirschner, K-wire fixation with sterilized, sharpened, smooth stainless steel pins has been the most available and forgiving technique for the fixation of most fractures and dislocations in the hand and wrist. K-wires have been widely used in bone operations due to their simplicity, reliability, and cost-effectiveness. According to a biomechanical study, K-wires offer a rigidity similar to interosseous wiring and other methods of fixation [1].
However, several reports have described complications resulting from the use of K-wires. Botte et al. [2] reported a complication rate of 18%, including pin loosening, pin tract infection, and pin bending. Although they were easily resolved by removal of the pin without permanent sequelae, some authors have described life-threatening complications, such as, distant migration to a vital organ [3].
Until now, no case report has described K-wire breakage due to a manufacturing defect. We describe the breakage of a K-wire during removal resulting in a permanently retained remnant in the medullary cavity.
A 15-year-old male was admitted to our hospital with right hand swelling and pain. Plain radiography revealed an oblique fracture in his right index metacarpal shaft with a dorsal apex angulation of 25 degrees. Under axillary block anesthesia, a tourniquet was applied to the upper arm at 250 mm Hg, and under fluoroscopic guidance, the fractured index metacarpal was reduced using the Jahss maneuver. The metacarpophalangeal (MP) joint and the proximal interphalangeal (PIP) joint were flexed at 90 degrees and upward pressure was applied on the flexed finger to correct dorsal apex angulation. After reduction, two 1.1 mm thick K-wires were inserted from the sides of the second MP joint to the metacarpal base. The locations K-wires were checked using a fluoroscope, and the distal sharp ends were cut to leave a 1 cm length of wire (Fig. 1). To immobilize the fractured segment, a short arm splint was applied. A week later, the short arm splint was removed and active range of motion was allowed. At 6 weeks postoperatively, radiologic union was achieved using plain radiography, and we attempted to extract the two K-wires. One of the K-wires was completely removed but the other broke at its mid-shaft (Fig. 2), leaving the remnant proximal portion buried in the medullary cavity (Fig. 3). Subsequently, the patient was able to flex and extend the MP joint fully and no symptoms such as pain, bleeding, or swelling were encountered. We noticed that the tip of the broken K-wire resembled the tip of the intact extracted wire. To determine the cause of the breakage, both K-wires were sent to the head office of the manufacturer (Solco Biomedical Co., Ltd., Pyeongtaek, Korea). We observed that the broken tip resembled the end of a normal K-wire tip in magnified view (40× magnification) (Fig. 4), signifying that the breakage was caused by a manufacturing defect.

A 15-year-old male had an oblique fracture on the shaft of the right second metacarpal. A plain radiograph taken 4 weeks after surgery shows the two K-wires placed after reduction of the right index metacarpal.
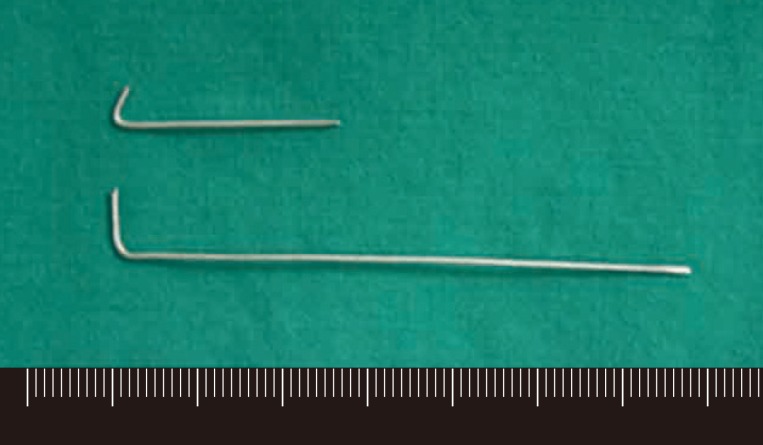
The two extracted K-wires. The upper one is the broken K-wire and the lower one is the normal K-wire.

Plain radiograph obtained at 6 weeks postoperatively, showing the residual K-wire portion in the medullary cavity.

The tip of the broken K-wire was relatively sharp and had the same angle as the normal K-wire (40× magnified).
K-wires are widely used for temporary fixation during hand fracture operations, and can be easily inserted and removed after bone union. K-wire fixation is a common and versatile method of achieving the internal fixation of fractures in the hand and wrist, and can be used to treat mallet finger and perform arthrodesis.
Nevertheless, complications of K-wire fixation have often been reported [2]. These complications could be classified as fracture-fixation-related or pin-related. The majority of fracture-fixation complications involve pin loosening due to poor initial pin placement. Accurate reduction and pin insertion must be confirmed by intraoperative X-ray fluoroscopy, and if loosening is recognized, the pin should be removed to reduce the risk of complications, which include infection, migration, and nerve and tendon injury. Pin tract infections, which are the most common pin-related complications, can be treated by preventing motion, oral antibiotics, and pin removal [4]. Osteomyelitis is a major complication of K-wire fixation. Botte et al. [2] observed the development of osteomyelitis from a pin tract infection in 1% of patients. Pin migration from a shoulder or upper extremity to the heart or major vessels has already been described by Lyons and Rockwood [3]. They reported 49 cases of K-wire migration, which included 17 to major vascular structures and 8 deaths, and found that the migration of K-wires used to fixate the shoulder girdle was responsible. Tendon injury has been reported infrequently. Botte et al. [2] described two cases of FDP tendon entanglement. Neurological complications can also occur. Gosens and Bongers [5] reported a neurological problem rate of 16.5% among 200 patients. All recovered without sequelae, though one with persistent radial nerve palsy required a graft from the sural nerve.
This report is the first to document K-wire breakage due to a manufacturing defect. It was difficult to identify the shaft defect responsible intraoperatively because the broken wire had an appearance similar to the normal wire. In fact, the defect was noticed only after pin removal and close examination of the broken tip.
K-wires are used for various functions, but are not always safe. Complications are an unavoidable consequence of surgical procedures, and thus, it is important to recognize their causes and prevent repeat incidents. Our experience in the described case cautions that potential complications resulting from K-wire defects should be borne in mind.
Notes
No potential conflict of interest relevant to this article was reported.