An Unexpected Complication after Periorbital Tumor Surgery in a Patient Later Discovered to Have Myelodysplasia
Article information
The myelodysplastic syndromes (MDS) comprise a complex group of stem cell disorders that involve the ineffective production of one or more of the myeloid class of blood cells. Patients with myelodysplasia often develop severe anemia and require frequent blood transfusions. One-third of thesepatients have a risk of developing acute myelogenous leukemia, usually within a few months to years of developing MDS. Thrombocytopenia is a common feature of MDS in which platelets mature abnormally. Bleeding in these patients is generally due to thrombocytopenia or intrinsic platelet dysfunction. The size, shape, and granulation of platelets are variable. Platelet aggregation is also impaired. The incidence of MDS is approximately 1 case per 1,000 people per year in patients who are more than 80 years old [1].
We encountered a case of a 94-year-old who presented with basal cell carcinoma (BCC) of the right medial canthus with a normal hematologic work-up and history (Fig. 1A). The preoperative hematologic work-up included a complete blood count, activated partial thromboplastin time, and prothrombin time.The patient had the current lesion for 3 years, and the lesion had been diagnosed as BCC with incisional biopsy 1 month before. She underwent excision with a wide margin (at least 5 mm of skin clearance) and full thickness, and immediate reconstruction with a forehead flap. Hemostasis was meticulously performed during the procedure. Within 4 hours of the operation, exaggerated ecchymosis, edema, and hematoma under the flap were observed (Fig. 1B). The hematoma was drained immediately, and the hematologic work-up was evaluated and detected to be above the minimum threshold. The bleeding time was prolonged (more than 10 minutes) clinically. A hematology consultation was requested, and the recommendations were performed. Based on a peripheral blood smear, MDS was diagnosed for the first time. Thirty units of platelet suspensions were given until the bleeding time reached the normal level (Table 1). Daily blood tests were repeated for 2 weeks postoperatively, and the signs and symptoms of bleeding and wound complications were observed closely. At the 3-week follow-up, the flap and the wound had a satisfactory appearance and had healed uneventfully, and the patient had no further bleeding episodes (Fig. 1C).
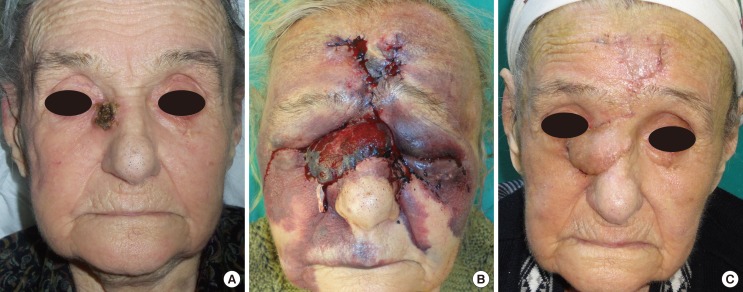
Views preoperatively (A), 4 hours postoperatively (B), and at 3-week follow-up (C).

A summary of the clinical situation in accordance with bleeding time and platelet level
Clotting disorders are an important cause of flap failure in reconstructive surgery. In patients with thrombocytopenia or an increased bleeding tendency, postoperative flap complications are well known [2,3]. The existing literature lacks reports of MDS patients undergoing reconstructive surgery, with only one report mentioning this clinical scenario. Murphy et al. [4] reported reconstruction of an extensive periorbital defect secondary to mucormycosis by free flap in a patient with previously diagnosed MDS. In this case, thrombocytopenia was controlled with thromboelastography (TEG). They concluded that the low platelet count implied a high complication rate. However, our case had normal platelet levels and underwent a minor intervention; this demonstrates that platelet dysfunction should be kept in mind in MDS treatment. In addition, this clinical scenario makes it difficult to diagnose MDS because a preoperative blood test cannot detect platelet dysfunction. It can only be determined by bleeding time test, thromboelastometry (TEM), and TEG, but these are not among the routine preoperative tests [5]. The authors suggest that in older patients, prior to surgery, a simple bleeding time test should be performed, even if the results of the laboratory tests are within the baseline values. If MDS is suspected, a hematology consultation and peripheral blood smear should be requested to search for MDS, or viscoelastic whole-blood assays such as TEM and TEG should be performed if possible, regardless of the size of the surgical intervention. Thus, the bleeding complications can be avoided, and the number of blood transfusions can be reduced. Nevertheless, if there is no possibility of TEG, a close monitoring of the bleeding time for detecting the amount of transfusion is still helpful.
Lack of experience can disrupt the provision of an optimal treatment plan for MDS patients. Upon the recommendation of hematologists, frequent platelet transfusions were given and a satisfactory outcome was achieved. This report proves the importance of closely monitoring the bleeding time and bleeding tendencies in these patients after surgery.
Notes
No potential conflict of interest relevant to this article was reported.