The Rat Model in Microsurgery Education: Classical Exercises and New Horizons
Article information
Abstract
Microsurgery is a precise surgical skill that requires an extensive training period and the supervision of expert instructors. The classical training schemes in microsurgery have started with multiday experimental courses on the rat model. These courses have offered a low threat supervised high fidelity laboratory setting in which students can steadily and rapidly progress. This simulated environment allows students to make and recognise mistakes in microsurgery techniques and thus shifts any related risks of the early training period from the operating room to the lab. To achieve a high level of skill acquisition before beginning clinical practice, students are trained on a comprehensive set of exercises the rat model can uniquely provide, with progressive complexity as competency improves. This paper presents the utility of the classical rat model in three of the earliest microsurgery training centres and the new prospects that this versatile and expansive training model offers.
INTRODUCTION
The increase in restrictions to animal use and the financial constraints of training in recent years have led to the development and spread of many non-living animal models for microsurgery simulation. Such models are numerous and include a huge spectrum such as rat cadavers, cryo-preseved rat aortas, chicken and turkey wings, leaves and grape skin, human cadaver vessels, and different styles of plastic simulation materials [1,2,3,4]. Most of these non-living models are sufficient in enabling students to acquire the basic set of microsurgery skills, especially in the early stages of training. At this beginner stage, the set of skills required includes a basic working knowledge of the surgical microscope, handling the microsurgery instruments and small sutures, and basic suturing and anastomosis techniques. Using non-living models for this purpose decreases the number of live animals used for training purposes, and gives students confidence when working with living tissues.
However, the live rat animal model remains an indispensable model for many training microsurgical courses around the world. The use of this model in microsurgery training stretches back to the early 1960's, when pioneers such as Lee [5] identified the need for low cost surgical models that could meet the clinical needs of the day. He and subsequent researchers went on to develop organ transplant models in the rat to help address the current immunological issues at that time. It became evident that there was a need to transfer these skills to the clinical sector, as these new microsurgical techniques opened up new surgical possibilities. This, in return, led to the establishment of microsurgical training courses utilizing the rat model across both shores of the Atlantic and the expansion of training [6].
THE DEVELOPMENT OF RAT-MODEL MICROSURGERY TRAINING COURSES: A TALE OF THREE CITIES
Many different microsurgery training courses have been successful in training surgical specialists from different specialties and countries. Even though they differ in their set-ups and programs, the basic curriculum is very similar, and we will briefly describe three of the longest serving courses using rats as a classical training model for microsurgery training: Paris School of Surgery (Paris, France), Northwick Park workshops (London, UK), and Columbia University (New York, USA).
The Paris School of Surgery is the longest serving out of eighteen training courses on the record to date in France, all of which are either basic 'certificate' courses or advanced university 'diploma' courses. The training lab was established in 1976 by Dr. Alain Gilbert, Gisèle Amichot, and Josette Legagneux as instructors. There is an in-house course manual [7], and the pedagogical approach designed at the beginning of the programme is still followed today. Currently, the course is directed by Professor Alain Masquelet. The course accepts an average of 60 students a year for its basic certificate training, and 50 students can take the advanced course (university diploma). The course teaches about 60-70 surgeons per year, and to date, the course has taught over 3,000 surgeons [8].
In the United Kingdom (working within Home Office guidelines for the use of animals), basic microsurgery workshops were established at Northwick Park Institute of Biomedical Research in 1979 by Professor Colin Green and Sandra Shurey, and over 3,000 surgeons have benefited from this training to date. A course manual was also written in-house to explain microsurgical theory and the use of the rat model, and to accompany the exercises incorporated into these workshops [9].
At Columbia University (CU), the Microsurgery Research and Training Lab was established in the early 1980s by Dr. Harold M Dick in the Department of Orthopedic Surgery, and now it is under the leadership of Dr. Melvin P. Rosenwasser and Dr. Yelena Akelina, training over 150 surgeons every year, from 12 specialties and more than 45 countries.
The three centres' basic courses are very similar, with slight variations, and here we note the common educational philosophy and style that is used. At the very beginning of the course, introductory videos and short lectures from the instructors are used to put students in the right mindset for learning and prepare them for the difficult and humbling experience of handling microsurgery for the first time. New techniques and exercises are introduced with a gradual increase in difficulty in parallel to the rise of students' confidence and frustration management.
All of the courses emphasise the importance of the right attitude and psychology set in achieving a successful outcome in microsurgery. All surgeons were first instructed on the use, care, and setup of the operating microscope, followed by basic interrupted suturing exercises on a rubber glove model to learn the difference between macro and micro-suturing. When this was mastered, the anaesthetised rat model was introduced.
In all courses, the rats are anesthetised intraperitoneally using a ketamine (75-95 mg/kg) and xylazine (5-8 mg/kg) cocktail and constantly monitored by the instructor and students for the depth of anesthesia. The rats' groin area is surgically prepared by standard methods and the femoral vessels are exposed, clamped, transected, and then anastomosed with 8 interrupted sutures using 10-0 nylon according to the standard methods of Acland [10].
Classical exercises were developed to take surgeons through a series of microsurgical maneuvers that would develop their skills in one week involving 35 to 40 hours of hands-on experience. All of the basic exercises utilised the femoral artery and vein, the epigastric artery and vein, and the sciatic nerve (Fig. 1). Surgeons would work at low- to mid -range magnification (×4-×15).
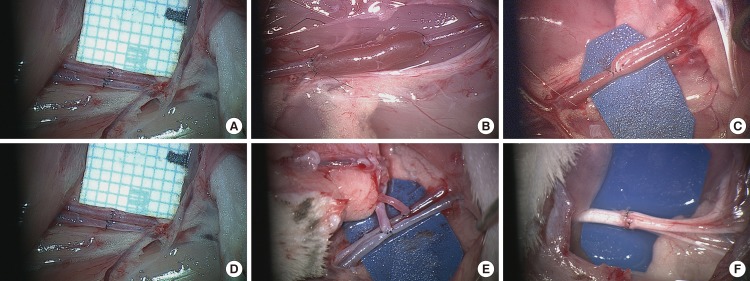
Basic rat model exercises
(A) The femoral artery and vein in the rat model. (B) Interpositional vein graft: femoral vein into femoral artery. (C) End-to-side anastomosis: femoral artery into femoral vein. (D) End-to-side arterial and venous anastomosis (groin flap). (E) Rat superficial inferior epigastric artery flap. (F) Rat sciatic nerve epineural repair.
The rat femoral area is used for basic exercises in preference to the aorta, carotid artery, or vena cava, as mistakes are easily managed and do not usually result in fatal hemorrhage. In the basic microsurgery skills course (3 days in Paris vs. 5 days in London and New York), surgeons learn how to prepare and care for the operative site, and how to prepare and care for micro-vessels ranging in size from 0.5 to 2 mm. They also perform interrupted suturing with 10/0 stitches on both individual end-to-end and end-to-side anastomoses using rat models of vein grafting and free flaps.
During the same time, students also learn how to safely apply clamps, the action to be taken if a clamp slips, and how to place stitches with a view to correct tension, bite sizes, and stitch placement according to the type of vessel, including how to remove stitches safely when necessary, as well as correctly interpreting patency.
RAT MODEL BASIC SKILLS COURSE COMPONENTS
Paris School of Surgery basic microsurgery course
In the basic course, students undergo 3 days of training (20 hours in total). Eight hours of the course is dedicated to theoretical lessons and 12 hours to practical training. During the course, the students learn how to use the microscope as well as six basic techniques of microsurgery, namely end-to-end anastomosis on synthetic and rat femoral vessels as well as vein graft to arterial defects (Fig. 1A, B). The training, however, is not sufficient for achieving competency. It is simply an introduction to microsurgery and its challenging techniques. Table 1 highlights the training exercises taught in this basic course.

Paris School of Surgery basic microsurgery course
London Northwick Park Institute for Medical Research (NPIMR) course
The Northwick Park basic microsurgery workshop runs over the course of one week (5 training days), utilizing the rat as its main training model. The exercises taught in this basic course (Table 2) include end-to-end rat femoral artery (approximate average diameter of 1 mm) and vein (approximate average diameter of 2 mm) (Fig. 1A); rat femoral vein graft into the femoral artery (2-mm vessel end-to-end into 1-mm vessel), which also involves surgeons learning how to cope with discrepant-sized vessels (Fig. 1B); end-to-side rat femoral artery into the femoral vein (1-mm vessel into 2-mm vessel) (Fig. 1C); rat groin flap (Fig. 1D, E) and nerve repair using the rat sciatic nerve model (2-mm epineural repair) (Fig. 1F). Some students go on to perform epigastric vein graft into femoral artery (1-mm vessel into 1-mm vessel, with a difference in vessel wall thickness) or even raise a groin flap on the epigastric artery (0.5 mm) and vein (1 mm) (Fig. 2A).

Paris School of Surgery advanced microsurgery (University Diploma) course
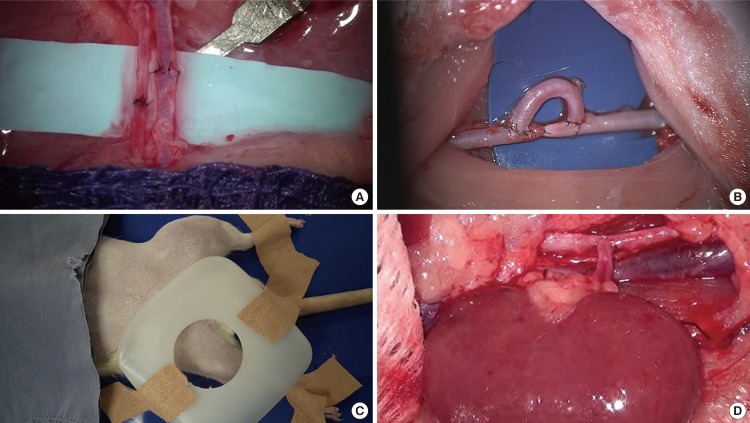
Advanced rat model exercises
(A) Rat epigastric artery and vein (diameter less than 1 mm). (B) Rat carotid artery loop (the femoral used as a graft-bypass). (C) A plastic dome simulator for anastomosis in a deep restrictive field. (D) The rat kidney autotransplantation exercise.
New York Columbia University basic microsurgery course
At Columbia University (CU), the basic microsurgery training course is also taught over 5 working days (40 training hours). As in Paris and London, the CU basic skills course consists of exercises for teaching the students basic microsurgery techniques such as end-to-end interrupted suturing of vessels using the rat femoral artery and vein model (Fig. 1A); interpositional vein graft (Fig. 1B); end-to-side anastomosis of arteries and veins that gives the student the ability to perform both arteriotomy and venotomy (Fig. 1C); and peripheral epineural nerve repair (Fig. 1F). However, there are a few extra points emphasised during the Columbia University course: 1) End-to-end arterial anastomosis (1 mm) is taught in both the conventional way as well as by one-way-up or the posterior-wall-first technique. 2) The course advocates the use of the inguinal fat pad as a hemostasis tool at the end of each exercise to reduce the bleeding time and to demonstrate the effect of fat tissue in hemostasis [11]. 3) The course stresses the need for the students to learn how to control anastomosis bleeding caused by gapping or uneven spacing without reapplying the approximating clamps in order to reduce the risk of thrombosis.
Table 3 highlights the training exercises taught in this basic course.

Northwick Park (London) basic course
RAT MODEL ADVANCED SKILLS COURSE COMPONENTS
Experienced surgeons who want to further develop their skills are encouraged to take the advanced courses available at all three centres, which also make use of the rat model.
Paris School of Surgery advanced microsurgery course
In this university diploma level advanced course, students are exposed to about twenty different training exercises on the rat. These include end-to-end anastomosis on vessels up to 1 mm in diameter (Fig. 2A), grafts (Fig. 1B), bypass (Fig. 2B), kidney transplantation (Fig. 2D), and a bundle of flap transfers (Fig. 1E). The course comprises 30 training sessions that run weekly over an 8 month period. In total, 120 hours of training is required to complete the training curriculum. The teaching method is based on stepwise increases in the difficulty of exercises. During the first 15 sessions, students do not repeat the same exercise. Rather, they practice a different more difficult technique every time. At the completion of the course, a final exam is applied, and a previous study showed that the success rate is related to the number of training hours [8]. Table 4 summarizes the training exercises taught in the Paris advanced course.

Northwick Park (London) advanced course
London Northwick Park Institute advanced course
This advanced microsurgical skills course is taught over a period of five days (40 hours). The exercises vary and are tailored to the students' ability and learning needs. As summarised in Table 5, the exercises taught routinely include micro-dissection skills in vessels below 1 mm (Fig. 2A); free tissue transfer using end-to-end and end-to-side anastomosis techniques (Figs. 1D, E, 2A); vascular grafts and bypasses (Figs. 1B, 2B); microvascular anastomosis in a deep restrictive area (Fig. 2C); vessel anastomosis without the use of double clamps; operation under maximum magnification (up to ×25); and continuous suturing. Additional specialised techniques taught to the candidates of specific specialties such as vasovasostomy, epididymovasostomy, and organ transplantation can also be incorporated.

Columbia University (New York) basic course
New York Columbia University advanced microsurgery course
At this institution, an advanced course for one week (40 hours) can be organized upon request. This course also utilises the rat model, and as in the London and Paris advanced courses, the rat model exercises are expanded and modified to teach students a bundle of advanced microsurgical techniques (Table 6). End-to-end anastomosis on a rat carotid artery, for example, gives the students the ability to work at different angles for suturing and various dissection skills. Interpositional vein grafts are taught with the rat epigastric vein (1 mm) inside the femoral artery (1 mm) to teach the handling of small vessels (supermicrosurgery). Furthermore, different free flaps, such as the rat groin flap, serratus anterior muscle flap, latissimus dorsi muscle flap, and myocutaneous flaps could be incorporated to teach the principles of free tissue transfer. Additional specialised exercises such as vasovasostomy and Fallopian tubal repair could also be included according to the student's specialty and specific goals associated with her/his surgical practice.

Columbia University (New York) advanced course
The following is a summary of the advanced exercises common to the three centres that they have developed to cover the skills training needs of the advanced trainees. These exercises can be an excellent foundation for higher skills necessary for clinical scenarios such as organ transplantation and complex chimeric flap reconstruction.
Renal transplantation
Renal transplantation in the rat incorporates meticulous dissection techniques, as it involves entwined vessels, different size disparities, vessel bifurcations, and differing orientations (vessel sizes 0.5-1 mm). This was first put forward as a microsurgical training model (using a slightly different model) by Korber and Kraemer [12] in 1988.
The transplant is performed end-to-end on the opposite renal vessels or end-to-side onto the infra-renal aorta and vena cava, which requires careful dissection skills, as the vena cava and aorta are in close proximity (Fig. 2D). Continuous stitching with 10/0 suture is performed, utilizing the front-wall-first or back-wall-first method (this simulates working in constricted areas where it is difficult to access the back wall). Continuous stitching was first recommended by Man and Acland [13] in 1981. It is faster, but the budding micro-surgeon must be aware of tension (particularly in veins), friability, bite size, and the possibility of catching the back/front wall.
The rat carotid loop
This exercise requires careful dissection skills and meticulous suturing. The carotid artery is entwined closely within a sheath containing small veins and the vagus nerve. The femoral artery is removed and anastomosed with 10/0 interrupted sutures in an end-to-side loop into the carotid (Fig. 2B).
Anastomotic techniques in a deep field (Fig. 2C) without the double clamp and at ×25 magnification (Fig. 2A)
Anastomosing in deep restricted areas is mimicked by the use of a plastic jig that fits over the rat femoral area. This gives an opening field 3 cm wide and 3 cm deep. A rat femoral artery and vein are then anastomosed end-to-end through this aperture.
Some clinical centres do not use or have access to double clamps, so the anastomotic techniques taught do not utilise this, and the rat femoral artery and vein anastomosis can be completed by starting at the centre of the back wall first or using a 1,200 or 1,800 orientation.
For very small vessels of 1 mm and below, a higher magnification is needed. Trainees learn that at this level of magnification, the light is not so bright and the depth of field is much shorter, meaning that the anastomosis must be carried out in a horizontal plane.
Rat groin flap models involve end-to-end anastomosis of the epigastric artery and vein (Fig. 1A). This exercise can be performed utilising an end-to-side anastomosis of these vessels onto the femoral artery and vein. The epigastric vein can also be anastomosed as a graft into the epigastric artery.
Vasovasostomy and epididymovasostomy
Rat models of vasovasostomy and epididymovasostomy are good substitutes for clinical operations due to their relatively large size in the rat, and are used routinely in vasectomy reversal workshops for urologists in the UK [7].
NEW HORIZONS IN MICROSURGERY TRAINING
Fifty years after Sun Lee's manual describing microsurgery techniques in the rat to address the needs of reconstructive surgeons of that time, the clinical world is again in need of further microsurgical training interventions with the advent of new horizons in microsurgery, namely, the advent of perforator flaps and lymphatic anastomosis. These new emerging techniques utilise vessels of below 1 mm. This has been termed 'supra-microsurgery' [14]. In addition, the use of microsurgical techniques is now being incorporated into many new areas of the clinical specialties. In 1979, most new micro-surgeons were from the field of plastic surgery. In contrast, current students come from a variety of specialties and include maxillo-facial, oral/otolaryngology (ENT), orthopaedic, hand, general, urology, obstetrics, paediatric, cardiac, and transplant surgeons.
When surgeons gain experience in microsurgery, the horizons for utilising the rat model are virtually endless, given the possibility to learn how to perform tail, toe, and organ transplants, to work with vessels with a size discrepancy, to work with video-assisted devices, to suture with continuous stitching, and other difficult exercises [15,16,17,18,19,20,21,22,23,24,25]. New techniques with the robot-assisted microsurgery open a new door to utilise the classic rat model for teaching surgeons from different specialties to perform microsurgical procedures using robotic arms. Other techniques and procedures that can be utilised in the rat for microsurgical training (but are yet to be permitted in the UK by current Home Office rules) include most of the organ transplants described by Lee [5] such as those of the liver, lung, small and large bowel, stomach, and pancreatico-duodenum. Additional exercises can include other free flaps, and muscle, bone, and limb transplantations.
CONCLUSIONS
It has been established that microsurgery training courses using rat models offer many advantages. They greatly enhance students' surgical skills and provide the highest fidelity simulator for clinical microsurgery. The use of rat models in advanced courses under a supervised training programme provides an excellent simulation model for complex microsurgical reconstruction procedures. As such, the rat model remains the best preparation for achieving high standards of competency in microsurgery. Advances in microsurgical reconstruction demand new educational interventions. The live rat is one of the most versatile models in microsurgery training courses worldwide, and 50 years after microsurgery was first pioneered, the rat model is still irreplaceable for advanced microsurgery skill acquisition. Its prospects include future educational roles in perforator flap techniques and robot-assisted microsurgery.
Notes
No potential conflict of interest relevant to this article was reported.