A Rare Form of Congenital Amniotic Band Syndrome: Total Circular Abdominal Constriction Band
Article information
Congenital amniotic band syndrome is a rare congenital abnormality with multiple disfiguring and disabling manifestations. A wide variety of clinical deformities are encountered, ranging from simple ring constrictions and minor digital defects to major craniofacial and visceral defects [1]. The abdomen is a rare location, and thus far, only a few cases of the abovementioned syndrome in the abdomen have been reported in the literature. Here, we report a child with a total circular congenital amniotic band of the abdomen, who was treated successfully by surgical excision.
A 9-year-old boy was referred to our clinic with deformity of the abdominal region. He was born to nonconsangineous parents at 32 weeks of gestational age by cesarean section. His family history and prenatal and natal histories were unremarkable. The circular constriction band of the abdomen was present at birth, and no other congenital abnormality was noted (Fig. 1). Magnetic resonance imaging of the abdomen showed an intact abdominal wall and normal visceral organs. The patient was operated under general anesthesia, and the fibrotic band, which was observed throughout the abdominal skin and the subcutaneous tissue, was resected, and multiple z-plasty flaps were performed. No postoperative complications were detected. Hypertrophic healing was noticed in some areas of the surgical scar probably due to the weight gain of the patient in the postoperative period. A silicone sheet was recommended. During the follow up, the patient had no complaint about the scar, so no further surgical intervention was planned (Fig. 2).
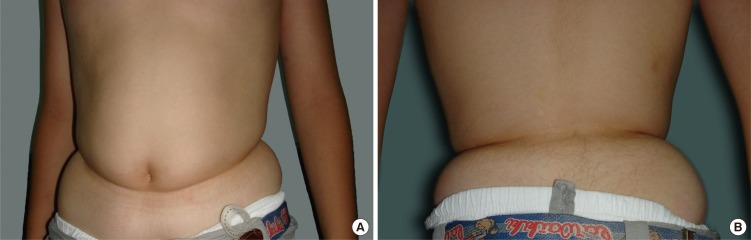
The circular constriction band of the abdomen. (A) Preoperative anterior view of the patient. (B) Preoperative posterior view of the patient.

Postoperative view. (A) Anterior view of the patient. (B) Posterior view of the patient.
A congenital constriction band is defined as a disorder present in a newborn infant, in which constriction rings or bands cause soft tissue depressions, encircle digits, extremities or limbs and rarely in the neck, thorax, and abdomen [1]. Familial occurrence is very rare, and there is no known genetic predisposition and/or gender difference. The pathogenesis is unknown; however, a number of theories suggest the etiology [1,2]. The intrinsic theory states that these deformities are a result of defective germ plasma within the embryo. In contrast, the extrinsic theory proposes that the lesions are caused by the strangulating action of the mesodermic bands, which are caused by an early rupture of the amnion. Amniotic bands are composed of either acellular fibrous tissue or fibrous tissue containing fibroblasts, covered by squamous cells [3]. The depth of a lesion varies from a shallow groove to a deep gutter and usually extends only up to the first fascial layer. Histology shows a grossly normal epidermis over a thickened dermis with collagen bundles and elastic fibers and large amounts of hyalinized connective tissue.
The circular constriction band of the abdomen is very rare. It was first reported by Brown et al. in 1957, and thus far, only 13 cases have been reported in the literature [3]. In most of these cases, the bands were above the pelvic rim, and the circular abdominal band was extremely rare [4].
The treatment of the circular constriction band can be accomplished by the removal of the fibrotic tissue with 1 to 2 mm of intact skin and by adding z-plasties or w-plasties to avoid further constriction of the scar. Subcutaneous tissue deficiency under the constriction ring can be corrected with rectangular plasty techniques and by using turnover dermofat flaps [5]. If the constriction is around the digits or extremities, urgent surgical treatment may be necessary because of vascular compromise. Otherwise, the treatment is usually performed for cosmetic reasons, and a staged correction may ensure the adequacy of vascularity to the residual limb or digit.
In conclusion, a circular constriction band of the abdomen is a rare congenital malformation and a rare form of amniotic band syndrome. Successful results can be achieved with the excision of the fibrotic band and the correction of the subcutaneous deficiency under the constriction. Children with amniotic band syndrome deformities should be referred for surgery early, particularly if there is vascular compromise.
Notes
No potential conflict of interest relevant to this article was reported.