Moll's Cyst Occurring in the Orbital Septum
Article information
Moll's cyst is one of the apocrine sweat gland cysts that occur on the margin eyelid. Thus far, however, only a few cases of Moll's cyst occurring in the orbital septum have been reported [1].
A 29-year-old woman complained of gradual swelling of the right upper eyelid. The patient had a history of undergoing blepharoplasty 7 years ago at another hospital. However, the patient had no other notable findings such as trauma. Upon physical examination, the patient was found to have a protruded mass when she had her eyes closed (Fig. 1). Ultrasonography revealed that the isoechoic mass was 1.6 cm×0.6 cm in size and had a well-defined margin and a fluid-containing lesion (Fig. 2). Under local anesthesia, we made a transverse incision along the double-eyelid line. The mass presented in the orbital septum. Through an incision of the orbital septum, we exposed the mass (Fig. 3). The mass was encapsulated by a transparent, white fibrous tissue. We carefully dissected it while paying special attention to not damage the levator aponeurosis. The patient wanted a mild blepharoptosis correction at the same time; therefore, we performed surgery on both eyes. Postoperatively, the mass contained a transparent fluid in the unilocular capsule. Histopathological examinations revealed that the tumor was composed of two layers of cuboidal epithelium. These two layers had a columnar shape (Fig. 4). Further, a 1-year follow-up revealed that the patient had no notable findings without recurrence (Fig. 5).
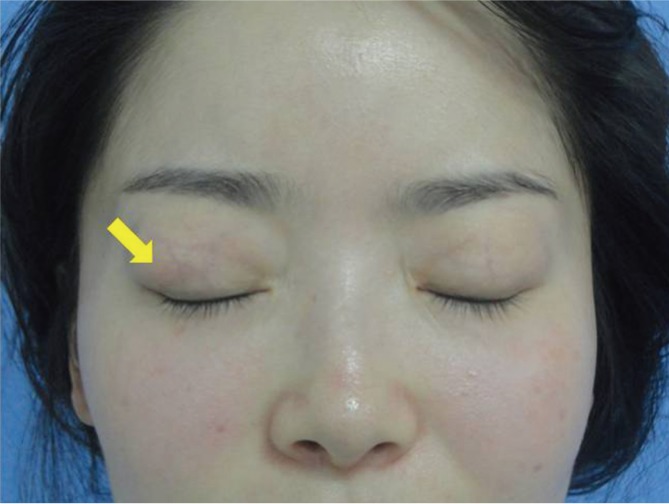
Preoperative findings: When the patient's eyes are closed, the protruded mass (yellow arrow) on the right upper eyelid becomes noticeable; this mass was soft, pliable, and round.
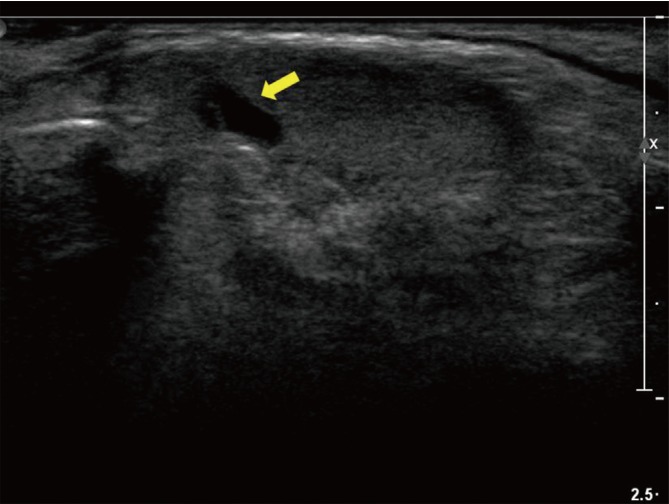
Preoperative ultrasonography: 1.6 cm×0.6 cm in size, an isoechoic mass with a well-defined margin and fluid-containing lesion (yellow arrow) on the lateral side.

Intraoperative findings. The cystic mass was in the orbital septum, surrounded by the periorbital fat. It contained fluid and was encapsulated by transparent, white fibrous tissue.
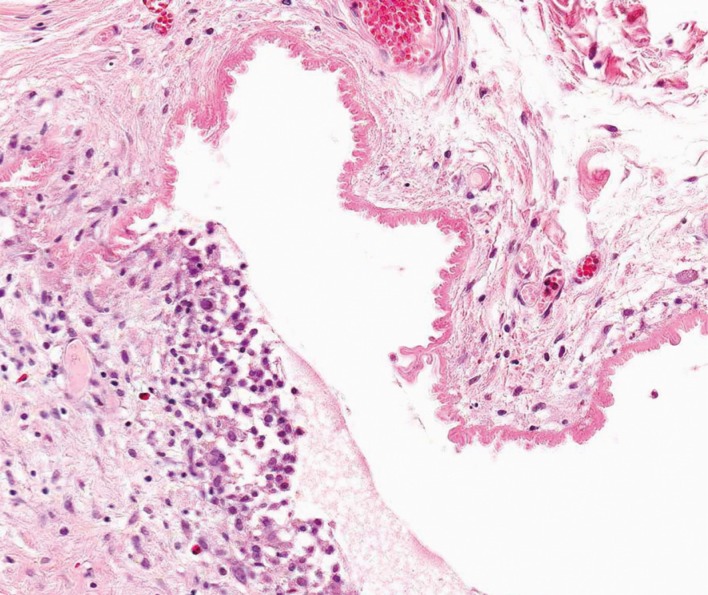
Histopathological findings. The tumor was composed of two layers of cuboidal epithelium surrounded by adipose fibrous tissue. The two layers of cuboidal epithelium had a columnar shape (H&E, ×200).

Postoperative findings (1 year later). The patient had no notable findings without recurrence.
Moll's cyst may also occur in the orbital septum because of congenital factors. That is, it occurs when there are disturbances in the development of the epidermis that should have developed on Moll's gland in the embryonic stage [2]. Further, it has been reported that Moll's cyst may also occur as a result of the epidermal invagination of the eyelid from certain acquired causes such as trauma or other iatrogenic factors [3]. Our case developed this cyst for acquired reasons and not congenital ones. This is attributed to the following:
Moll's cyst occurs very rarely in the orbital septum.
Concurrent deformities of the adjacent tissue may also occur during the growth to the adult stage in congenital cases of Moll's cyst.
The patient complained of the discomfort on the eyelid only recently.
The patient had a history of blepharoplasty.
Moll's cyst is surrounded by a thin white wall and contains a transparent fluid. Histologically, a cuboidal epithelium composed of two layers of secretory cells forms the inner wall of the cyst, and the rest of the cyst undergoes a fibrotic change. Of the two layers of secretory cells, the inner layer is composed of columnar epithelium and protrudes into the cyst. Further, its apical portion contains an eosinophilic substance. These findings are similar to those of Moll's gland [4]. In the current case, the clinical characteristics and histopathological findings were typically suggestive of Moll's cyst. In other words, we witnessed a rare case of Moll's cyst occurring in the orbital septum.
Notes
This study was presented at the 31th Korean Society for Aesthetic Plastic Surgery on April 27-28, 2013, in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.