Chondromyxoid Fibroma of the Finger
Article information
A 35-year-old man visited us with a chief complaint of painful swelling of the finger. A physical examination revealed a palpable mass, measuring approximately 2 cm×1 cm, on the dorsoradial side of the base of the middle phalanx of the right index finger (Fig. 1A). Upon history taking, we found that the mass had formed 7 to 8 years before and had since grown slowly. The mass had a firm, hard, discrete, and immobile consistency. An X-ray revealed a translucent, osteolytic lesion at the base of the middle phalanx; this lesion was eccentrically located to the cortex (Fig. 1B). The lesion was a mass with an ovoid shape and was parallel to the long axis of the bone; it had a slightly marginal sclerotic border. Moreover, it exhibited expansile growth to the adjacent soft tissue on the dorsoradial side. On the basis of these findings, we made a 2-cm straight, longitudinal incision on the radial side of the dorsum of the middle phalanx, thus confirming the presence of a bulging well-circumscribed cartilaginous-appearing mass (Fig. 2A). We performed an extensive, aggressive curettage of the lesion. The resulting bony defect was filled using iliac bone graft and screw fixation. In the resected specimen, there was a yellowish-white lobulated mass of 2 cm×1 cm×1 cm in size (Fig. 2B). On histopathological examination the mass mainly had a myxomatous appearance and was characterized by the lobular arrangement of stellate or spindle-shaped cells. The lobule was well circumscribed by fine fibrous septa and was composed of the central hypocellular area and the peripheral hypercellular area (Fig. 3). On the basis of these findings, we established a diagnosis of chondromyxoid fibroma (CMF). In the 15-month postoperative follow-up, the patient underwent an uneventful course without recurrent or metastatic episodes.
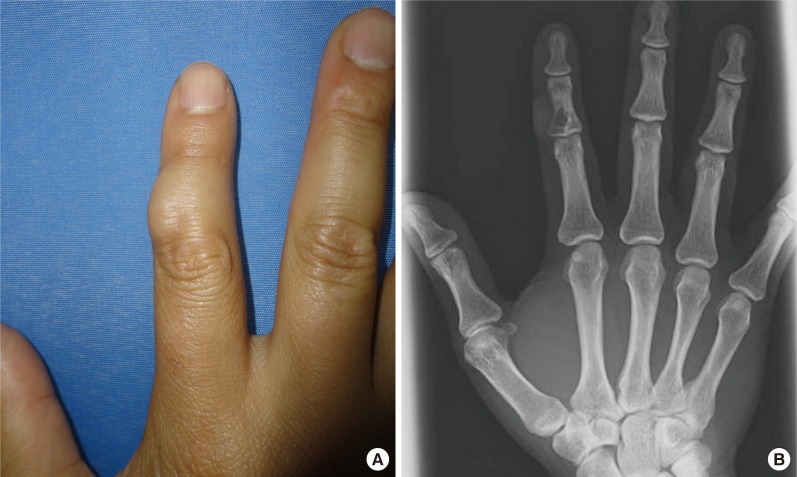
Preoperative findings. (A) Clinical photograph of the right index finger with a visible mass protruding from the dorsoradial side of the middle phalanx. (B) Preoperative anteroposterior X-ray film of the right index finger reveals radiolucent tumor in the metaphyseal-diaphyseal area of the middle phalanx.
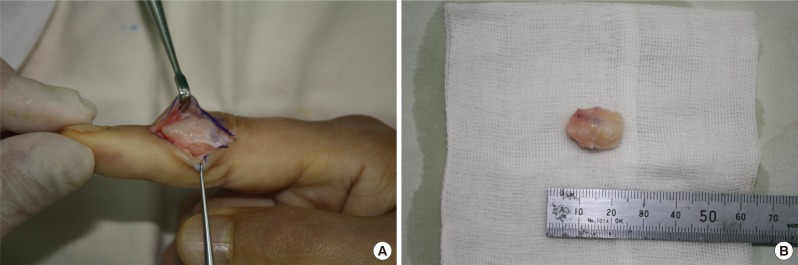
Intraoperative findings. (A) Incision planning with exposure of the mass. (B) Resected specimen (2 cm×1 cm×1 cm).
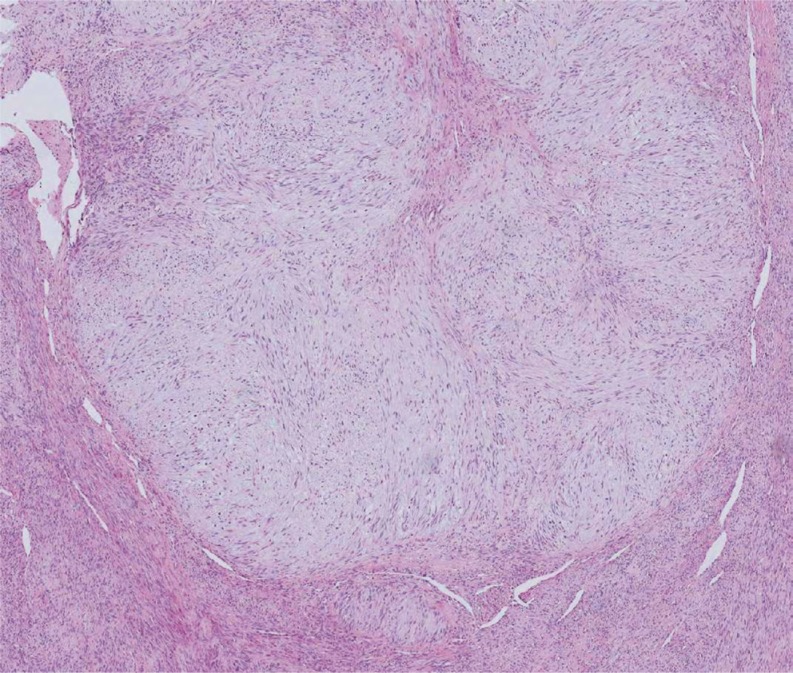
Histopathology and immunohistochemistry findings. The tumor shows alternating hypocellular and hypercellular areas. The hypocellular areas form lobules composed of loosely arranged cells in the gray-blue chondromyxoid matrix and surrounded by hypercellular spindle cells (H&E, ×40).
CMF was first described by Jaffe and Lichtenstein in 1948, and it is a rare, slowly growing benign bone tumor of cartilaginous origin. It accounts for less than 1% of all the primary bone tumors and less than 2% of benign bone tumors. Approximately 80% of the total cases occur in individuals aged 36 years or younger. There is no gender-related difference. To date, no definite etiologies have been documented. It is known that approximately 75% of the total cases of CMF affect the bones of the lower extremities. In particular, it occurs most frequently in the tibia and femur around the knee joint. Thus far, its incidence in the hand has been described to be very rare. Most cases of CMF typically originate from the metaphysis and may then extend to the epiphysis and diaphysis. The most common clinical manifestations of CMF include swelling and pain at the sites of primary tumor growth, but there are also some asymptomatic cases. Plain radiography shows that CMF has a round-to-oval medullary lesion with a well-defined margin and is parallel to the long axis of the bone. The tumor with a thin scalloped, sclerotic border has an eccentric location in the metaphysis and a translucent, osteolytic, bubbly appearance. Furthermore, it shows a slightly expansile growth to the adjacent soft tissue. For establishing the diagnosis of chondromyxoid fibroma, histopathological examinations are essential. In a nutshell, CMF is a firm, white, lobulated, well-circumscribed solid tumor mass that is sharply demarcated from the adjacent bone marrow. Light microscopy revealed that CMF is composed of three zones: myxomatous, fibrous, and chondroid zones. Histopathologically, it is characterized by the multilobular arrangement of stellate or spindle-shaped cells in an abundant myxoid background or chondroid intracellular material. These lobules are composed of the central hypocellular area and the peripheral hypercellular area. Surgical excision is the first-line choice for chondromyxoid fibroma, for which only simple curettage is performed or a bone graft is used for filling the cavitary defect following curettage. Although variable depending on the reports, the recurrence is estimated at approximately 25%. Postoperatively, regular follow-up including radiography is necessary. A good prognosis of CMF has been documented. In addition, it has been reported that CMF shows no distant metastasis [1,2,3,4,5].
Notes
No potential conflict of interest relevant to this article was reported.