Clinical Experience with Treatment of Angioleiomyoma
Article information
Abstract
Background
Angioleiomyoma, a vascular leiomyoma, is a rare, benign smooth-muscle tumor that originates in the tunica media of vessels. It occurs anywhere in the body, most frequently in the lower extremities.
Methods
We reviewed the medical records of 16 patients who were treated for angioleiomyoma between 2000 and 2012. The clinical features of angioleiomyoma and the correlation between symptoms and pathological subtypes were investigated.
Results
There were 9 males and 6 females. Ages of the patients ranged from 21 to 61. Pain was the primary symptom in 44% of the patients. Tumors were smaller than 2.0 cm in all dimensions and were located in the face in 4 patients, whereas 5 lesions occurred in the upper extremities and the remaining 7 in the lower extremities. Three histologic subtypes were identified: solid, venous, and cavernous. The subtypes did not correlate with the clinical symptoms.
Conclusions
Angioleiomyoma appears to be a rare tumor that occurs in the face and the extremities. The tumor usually occurs in middle age. A differential diagnosis of this tumor is difficult, but the tumor should be considered in the diagnosis of painful subcutaneous masses. Ultrasonography and magnetic resonance imaging can be helpful in the diagnosis of angioleiomyoma. These tumors can be successfully treated with simple excision, with a low recurrence rate.
INTRODUCTION
Angioleiomyoma, also known as vascular leiomyoma, is a rare, benign, solitary tumor that originates from the vascular smooth muscle (tunica media). It usually presents as a painful nodule in 30- to 50-year-old subjects. Angioleiomyoma can be found anywhere in the body, although it is more frequently located in the lower extremities [1,2]. This tumor is rarely diagnosed until it is excised and a histopathological examination is conducted. In 1973, Morimoto [3] classified cases of angioleiomyoma into 3 histologic types: solid, venous, and cavernous. He also divided the cases into a larger group of extremity tumors and a smaller group of head tumors and mentioned that the former consisted mainly of the solid type of tumors and are often painful, whereas the latter consisted of tumors that are usually venous and painless. However, correlations between clinical presentation and pathologic types, if any, have not yet been ascertained. We reviewed 16 consecutive patients who were treated at our facility over the last 12 years in order to investigate correlations between clinicopathological features and pathological types of angioleiomyoma.
METHODS
We retrospectively analyzed the medical records of 16 patients with angioleiomyoma who were treated in our hospital between March 2000 and July 2012. All patients underwent simple excision of the tumor. Diagnoses were based on the results of a pathological examination of the specimens. The surgical specimens were stained with hematoxylin and eosin stain. Variables selected for the analysis were age, sex, anatomic location, size, symptoms, preoperative diagnosis, coexisting disease, and recurrence. The follow-up period ranged from 6 to 18 months. Patient characteristics were analyzed using PASW ver. 18.0 software (SPSS Inc., Chicago, IL, USA), and the significance of differences was determined through nonparametric methods, namely, the Mann-Whitney U Test and the Wilcoxon W test to identify differences between patients' demographic data and the chi-squared test in order to determine whether differences between histological findings and clinical presentations were significant. A P-value of less than 0.05 was considered statistically significant.
RESULTS
Of the 16 patients in the series, 9 were male and 7 were female, yielding a ratio of 1.3:1. The median age of the patients was 8 years (range, 21-61 years), and most of the patients were in their sixth decade of life (Fig. 1). Gender differences existed in the ages of patients, with males (median, 53 years; range, 44-61 years) older than females (median, 38 years; range, 21-54 years) (P<0.05). The tumors were located in the face in 4 patients, whereas 5 lesions occurred in the upper extremities and the remaining 7 in the lower extremities. Pain was the most characteristic subjective complaint, reported in 7 (44%) of the patients. This pain was usually described as paroxysmal, drilling, and radiating, and it was often related to touch. The tumors that occurred in the face were not accompanied by pain.
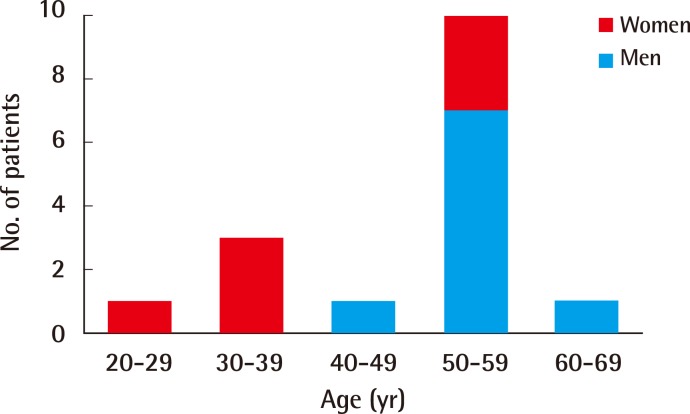
Ages of the 16 patients with angioleiomyoma
Some preoperative ultrasound examinations revealed well-defined, low echoic, hypervascular nodules with homogenous structures, suggesting benignity (Fig. 2). Preoperative diagnoses included ganglion, neuroma or neurilemmoma, inclusion cyst, and lipoma. All were incorrect, and none of the cases were diagnosed clinically as angioleiomyoma. The clinical data are summarized in Table 1.
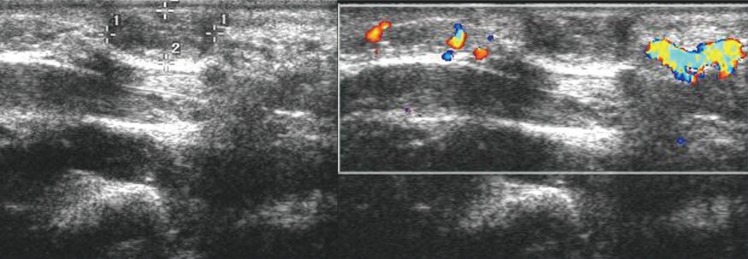
Ultrasound image of case 13
Ultrasound examinations revealed well-defined, hypervascular nodules, suggesting benignity.

Clinical charateristics in 16 patients with angioleiomyoma
Each tumor was removed by simple excision and primary closure of the defect. On excision, 16 tumors were found to be between 0.5 cm and 2.0 cm in all dimensions (median, 1.0 cm). The size of the lesions differed significantly between the symptomatic group (median, 1.0 cm; range, 0.8-2.0 cm) and the asymptomatic group (median, 0.7 cm; range, 0.5-2.0 cm) (P<0.05). Macroscopically, two were irregular and lobulated structures, while the remaining 14 were smooth, rounded, and well-encapsulated. The cut surface was glistening and gray-white or reddish-brown, the latter hue probably due to the large number of blood vessels.
A histological examination revealed well-demarcated nodules in the deep dermis. The nodules consisted of thickened smooth muscle fibers and vascular channels surrounded by thin capsules. Organizing thrombis, mature fat cells, and lymphocytic infiltrates were found in some tumors. Small areas of hyaline or myxoid changes were observed focally in 3 cases. According to the histological classification, the 16 cases of angioleiomyoma were categorized into 3 types: solid (n=5, 31%), venous (n=8, 50%), and cavernous (n=3, 19%). Some patients (4 cases) had a coexisting mass (Table 1). A physical examination was conducted as part of each of the follow-up visits after surgery, and no recurrences were reported in any cases.
Case 13
A healthy, right-handed 55-year-old man with no antecedent trauma presented with a 30-year history of a slowly growing and tender mass in the dorsum of the right hand. The mass was soft and freely movable and was 1.5 cm in diameter. It was not transilluminated. The overlying skin was raised but not thinned or discolored (Fig. 3).

Preoperative photograph of case 13
Preoperative appearance of a soft and movable nodule (diameter: 1.5 cm) on the right hand dorsum.
He underwent simple excision of the mass under local anesthesia. A discrete nodule 1.5 cm×1.2 cm×0.8 cm in size was detected in the subcutaneous tissue. The tumor appeared to be a grossly homogeneous pearly-gray nodule (Fig. 4). Its histological features were consistent with angioleiomyoma, showing thickened smooth muscle fibers and blood vessels (Fig. 5).
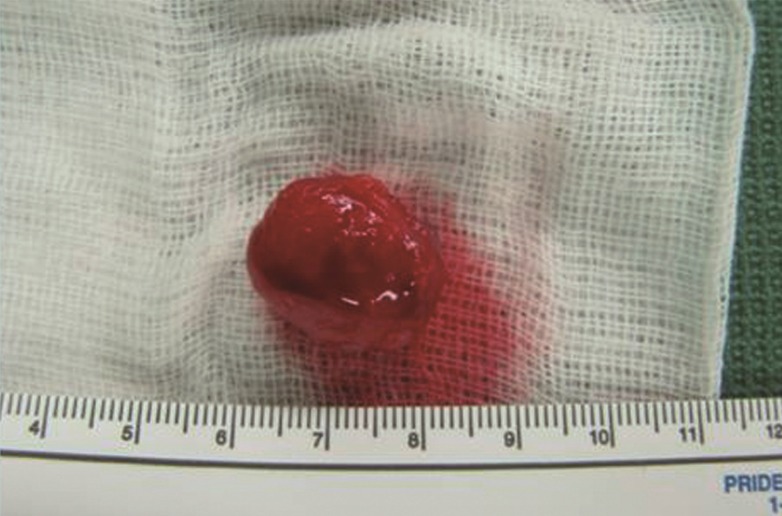
Intraoperative photograph of case 13
Intraoperative view showing an excised solid, pearl-gray discrete nodule.
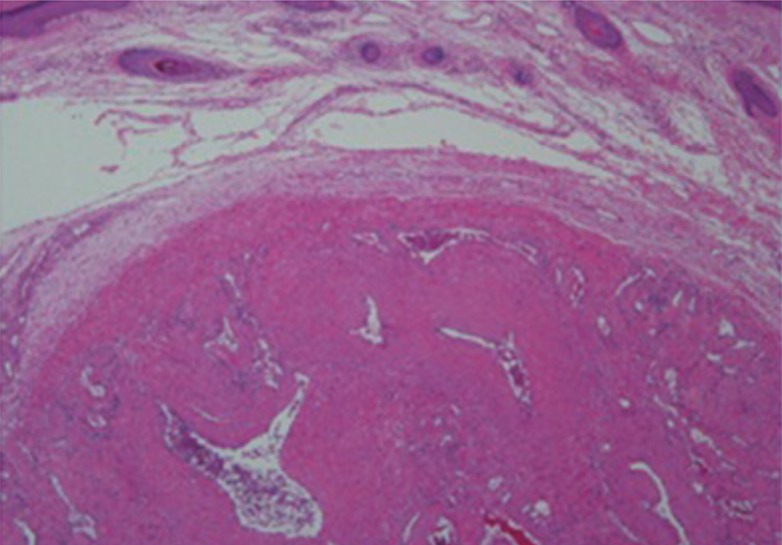
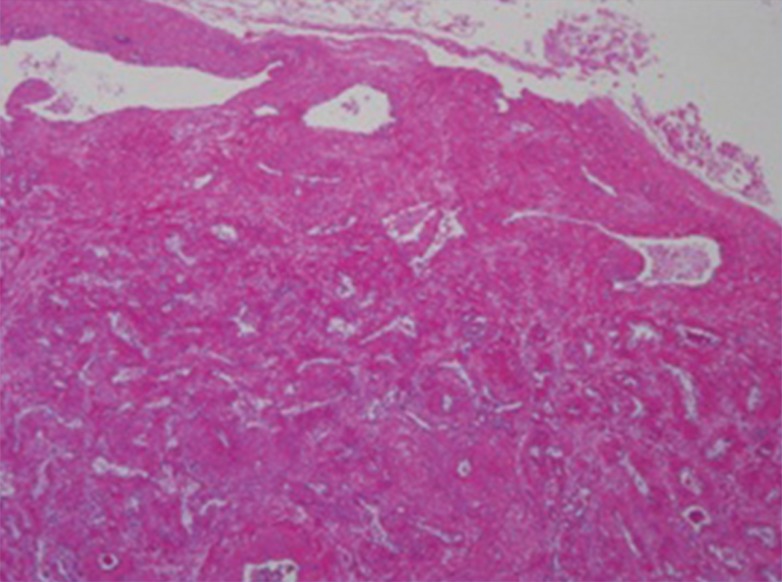
Pathologic photograph of case 13
A nodule containing thickened smooth muscle fibers and blood vessels. Irregular lumina of veins are noted (H&E, ×40).
Case 15
A 61-year-old man presented with an unusual lesion on the right soft triangle of the nose (Fig. 6). The mass was a, painless, slow-growing mass 1.0 cm×0.5 cm in size, and the patient had noted the mass several years prior to this presentation. Preoperatively, the presumptive diagnosis was a vascular malformation. The mass was resected, and composite grafting from the right postauricular skin was performed. A microscopic examination of the pale brown specimen revealed that the lesion was an angioleiomyoma. The histological findings indicated variably sized blood vessels mixed with smooth muscle bundles (Fig. 7).

Preoperative photograph of case 15
Preoperative appearance of a mass on the right soft triangle of the nose.
Pathologic photograph of case 15
A mass containing variable-sized blood vessels mixed with smooth muscle bundles. The thick walls of the blood vessels are indicative of the venous subtype of angioleiomyoma (H&E, ×40).
DISCUSSION
Angioleiomyoma is a rare, benign, smooth muscle tumor arising from the tunica media of veins and is seldom diagnosed before surgery. Angioleiomyoma can be found throughout the body but occurs most frequently in the lower extremities [1,2,3,4,5,6]. It commonly arises in the dermis or subcutaneous tissue [2]. A majority of these tumors are quite small, generally less than 2 cm in diameter [1,2,3,4], which is consistent with our results.
Our review also supports previous results that indicated that angioleiomyoma is usually seen in patients aged between 30 years and 60 years [1,2,3,4,5,6,7,8]. The male patients were significantly older than the female ones. Our sex distribution, a male-to-female ratio of 1.3:1, has not been seen in any previous study because angioleiomyoma has a female preponderance [1,2,3,4,5,6].
Classically, the most evident symptom of angioleiomyoma is pain with or without tenderness that is often paroxysmal in nature and precipitated by light touch, by exposure of the tumor to wind or cold, or by other imperceptible stimuli [1,2]. Pain and/or tenderness may be the presenting feature in 45% to 70% of all cases [1,2,3,4,5,6,7]. Patient ages in the symptomatic group and in the asymptomatic group did not differ significantly. The percentage of symptomatic males (44%) did not differ significantly from the percentage of symptomatic females (43%).
Angioleiomyoma can be classified into 3 types: capillary or solid, cavernous, and venous. Hachisuga et al. [1] reported that in their series of angioleiomyoma cases, the solid type was most common (66%), followed by the venous (23%) and then, the cavernous (11%) types. This is inconsistent with our results-in our study, the venous type (8 cases) was most common, followed by the solid type (5 cases) and then, the cavernous type (3 cases). However, they stated that in females, the solid type occurred most frequently, particularly in the lower extremities, which is consistent with our result. They also mentioned that in males, tumors of the venous type developed most frequently as opposed to our study in which tumors of the cavernous type were most common and in which the upper extremity and head were involved more frequently in males than in females.
In our study, we could not demonstrate any correlations between histological findings and clinical presentation. There were no statistically significant correlations between the histological types and the pain symptoms (P>0.05). Our results are thus in disagreement with those of Hachisuga et al. [1]. However, our study showed that in the head region, the tumors usually made elicited no pain symptoms, which is consistent with the results of Hachisuga et al. [1]. Angioleiomyomas occurring in the hand are less painful, and not predominantly of the solid type nor predominantly seen in the lower limbs [8]. The pain can be caused by local ischemia from the contraction of the tumoral vessels [3]. A recent immunohistochemical study has demonstrated that the pain may be mediated through nerve fibers, particularly within the tumor parenchyma [6]. Small nerve fibers can be identified within the capsule of the tumor and tumor stroma in most cases, irrespective of the histological subtypes.
It is difficult to make differential diagnoses between angioleiomyomas and other tumors. Angioleiomyoma should be considered in lesions of the extremities, such as ganglions, fibroma, lipoma, glomus tumors, neurofibroma, and cysts [7,8,9,10]. Ultrasonography and magnetic resonance (MR) imaging can be helpful in the diagnosis of angioleiomyoma. An ultrasound examination revealed that angioleiomyoma shows well-defined margins and a homogenous structure, suggestive of the benign nature of the lesion [7]. MR findings are also relatively nonspecific, but T2-weighted images show a mass with mixed areas that are both hyper- and isointense relative to the skeletal muscle and a hypointense rim [9,10]. However, with a high index of suspicion and awareness, a preoperative diagnosis is possible.
Excision of an angioleiomyoma is simple and is the treatment of choice. Morbidity is minimal, and recurrence has been reported in only a few cases [1]. Malignant variants of this tumor, either as primary vascular leiomyosarcoma, or as malignant recurrence of a preexisting angioleiomyoma, are quite uncommon and account for 7% of all soft tissue sarcomas [11].
Taken together, after reviewing our patients with angioleiomyomas, we obtained the following results: 1) Angioleiomyomas had a similar sex distribution. 2) They occurred frequently in middle-aged persons. 3) They more frequently affected the lower extremity in females. 4) They more frequently affected the head and upper extremities in males. These results were compatible with the results of previous reports. Angioleiomyoma is difficult to diagnose before surgery despite the presence of these clinical manifestations. Thus, angioleiomyoma should be included in the differential diagnosis of painful nodular lesions.
Notes
No potential conflict of interest relevant to this article was reported.