Implications of abnormal abdominal wall computed tomographic angiography findings on postmastectomy free flap breast reconstruction
Article information

Abstract
Background
Preoperative computed tomography angiography (CTA) of the abdominal wall vessels is used when planning free flap breast reconstruction (FFBR) because it provides a surgical road map which facilitates flap harvest. However, there are few reports on the effect of abnormal findings on the operative plan.
Methods
We conducted a retrospective study of all FFBRs performed at a tertiary referral center over a 6-year period (November 2011 to June 2017). One consultant radiologist reported on the findings. Details on patient demographics, CTA reports, and intraoperative details were collected.
Results
Two hundred patients received preoperative CTAs. Fourteen percent of patients (n=28) had abnormal findings. Of these findings, 18% were vascular anomalies; 36% tumorrelated and 46% were “miscellaneous.” In four patients, findings subsequently prevented surgery; they comprised a mesenteric artery aneurysm, absent deep inferior epigastric (DIE) vessels, bilateral occluded DIE arteries, and significant bone metastases. Another patient had no suitable vessels for a free flap and the surgical plan converted to a pedicled transverse rectus abdominis musculocutaneous flap. The remaining incidental findings had no impact on the surgical plan or appropriateness of FFBR. More than one in 10 of those with abnormal findings went on to have further imaging before their operation.
Conclusions
CTA in FFBR can have a wider impact than facilitating surgical planning and reducing operative times. Incidental findings can influence the surgical plan, and in some instances, avoid doomed-to-fail and unsafe surgery. It is therefore important that these scans are reported by an experienced radiologist.
INTRODUCTION
Deep inferior epigastric perforator (DIEP) flaps are the current gold standard in autologous breast reconstruction due to the large amount of well-vascularized tissue that can be reliably harvested from the lower abdomen with minimum morbidity [1]. The anatomy of the deep inferior epigastric (DIE) vessels has been well documented [2]. Preoperative computed tomography angiography (CTA) of the abdominal wall vessels is frequently used when planning free flap breast reconstruction (FFBR) because it provides a surgical road map allowing surgeons to familiarize themselves with the patient’s vascular anatomy prior to surgery [3-5] and reduces operative time [6-8]. The most suitable perforator(s) can be identified, their courses through the rectus muscle determined, and their location from the umbilicus and abdominal midline quantified.
Previous studies have noted that computed tomography (CT) imaging can lead to the discovery of incidental and abnormal findings [9,10], the former often called “incidentalomas,” although this term is misleading due to the implication of the tumor-related suffix. These are unexpected lesions or masses found on CT imaging performed for other reasons. Incidental findings can be categorized by clinical relevance: major (findings that might alter the patient’s clinical course), moderate (findings where follow-up is sufficient), and minor (not influencing the patient’s course) [10,11]. Whilst, there are few reports on the prevalence of incidental findings [12,13] in FFBR, there are few that discuss the effect on the subsequent operative plan and management [14,15]. Additionally, the benefits of CTA must be weighed against the sizeable expense and radiation exposure.
The aim of this study was to identify the prevalence of incidental abnormal findings in our patient population and assess the clinical and financial significance of these findings.
METHODS
This study was part of a quality improvement assessment and an ongoing departmental free flap audit within our hospital. Audits and quality improvement assessment are part of a larger framework for clinical governance, whereby National Health Service (NHS) organizations are accountable for continuously improving the quality of their services and safeguarding high standards. Clinical governance (inclusive of audits and quality improvement assessments) is compulsory within the NHS. In addition, all data were collected retrospectively from hospital medical records. Under the Caldicott principles, non-identifiable patient data can be collected, stored, and used for purpose of audit without individual patient consent. No specific ethical committee approval is therefore needed. Subjects in clinical photographs gave informed consent for use of images.
A retrospective cohort study was performed on all DIEP FFBRs performed at a tertiary referral hospital who received a preoperative CTA over a 6-year period (November 2011 to June 2017). One consultant radiologist (BCK) reported on the findings to reduce inter-reporter variability. Incidental findings were defined as masses or lesions that differed from normal anatomy found by coincidence during CT angiography, as in similar studies [15].
Details on patient demographics, CTA reports, and intraoperative details were collected retrospectively from hospital records. The data were tabulated in Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and analysis completed with IBM SPSS Software version 24.0 (IBM Corp., Armonk, NY, USA). Data were analyzed using the Kolmogorov-Smirnov test; age and body mass index (BMI) were found to follow a normal distribution and so the Student t-test was used to measure differences between data. Time from CTA study date to operation date did not follow a normal distribution and the Mann Whitney U-test was used to measure differences in non-parametric data, such as time from CT imaging date to operation date.
RESULTS
A total of 200 patients underwent preoperative CTAs prior to their proposed abdominal flap breast reconstruction. Patient demographics and operative details are shown in Table 1. The mean age of patients with abnormal findings was statistically similar to those without (51 years vs. 50 years, P = 0.665), as was BMI (27.5 kg/m2 vs. 27.3 kg/m2, P = 0.821). All flaps survived.
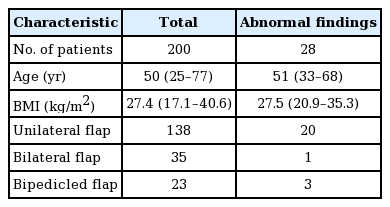
Patient characteristics and operative details
Abnormal incidental CTA findings were found in 28 cases (14%) (Fig. 1); five (18%) of which were vascular, 10 (36%) were tumor-related, and 13 (46%) were classified as “miscellaneous” as described in Fig. 2. Benign liver lesions were the most common unexpected finding. Eighteen percent (n = 5) of the incidental CTA findings (3% of all 200 patients) had major clinical relevance. Four patients had their surgery cancelled because of those findings (Table 2). These findings consisted of a mesenteric artery aneurysm, absent DIE vessels, bilateral occluded DIE arteries, and significant bone metastases (Figs. 2 and 3). One patient had their free flap procedure converted to a pedicled transverse rectus abdominis musculocutaneous (TRAM) flap and this case is described below.
Types of abnormal findings
Types of incidental findings found within our patient cohort. DIEA, deep inferior epigastric arteries.
Iliac crest metastases on CTA
(A) shows transverse computed tomography image with a large iliac crest metastasis circled. (B) is nuclear bone scintigram with increased uptake in the iliac crests signifying metastases of the same patient. CTA, computed tomography angiography.

Cause of cancelled operations
Mesenteric artery aneurysm
(A, B) A three-dimensional reconstruction of computed tomography angiography image illustrating a large mesenteric artery aneurysm found incidentally on the preoperative imaging.
In the remaining 23 cases, the incidental findings were not of major relevance and did not affect the decision to proceed to surgery. However, 9% (n = 2) were of moderate clinical relevance (1% of all 200 patients) and went on to have further imaging before surgery as described in Table 3. Liver lesions were the abnormal finding most commonly investigated further. Three quarters of the abnormal findings (n = 21) were of minor clinical relevance, i.e. there was no delay or change in reconstructive plan or follow-up required.
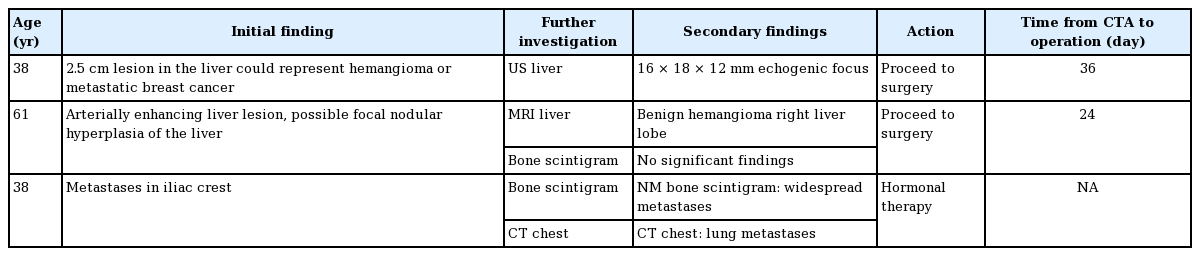
Further imaging in patients with incidental CTA findings who proceeded to surgery
The median time from date of CT imaging to operation date for all patients was 15 days (range, 1–235 days), which did not differ significantly between patients with incidental findings and those without (15 days vs. 15 days, P = 0.631; Mann Whitney U-test).
Illustrative case
A 65-year old non-smoker (BMI, 35 kg/m2) was referred for tertiary breast reconstruction post radiotherapy to salvage a painful and contracted implant-only reconstruction. This patient had a severe grade 4 capsular contracture with scarring and deformity to the abdomen from previous surgeries (Fig. 4). A left free hemi-DIEP flap was planned, however, CTA showed absent left DIE vessels so the operative plan was changed to a two-stage surgically delayed pedicled TRAM flap.
Preoperative images of illustrative case
A 65-year old woman was referred for breast reconstruction to salvage a painful and contracted implant-only reconstruction. Please note the severe post-radiotherapy grade 4 capsular contracture with loss of volume and skin. The extensively scarred abdomen is from multiple previous operations. (A) Frontal view and (B) profile view.
At the first stage, surgical flap delay was performed by incising down to rectus fascia at the superior and inferior borders of the flap, and partially raising both halves of the abdomen up to the lateral row of the perforators then replacing the flaps back to their natural positions. Immediate post first stage images are seen in Fig. 5. The second stage was performed five weeks later comprising total capsulectomy with implant removal and inset of a left pedicled hemi-TRAM flap. The flap transfer was successful with no partial flap necrosis or wound breakdown at the donor or recipient sites, and the patient had good symmetry compared to contralateral breast tissue (Fig. 6).
Five-week postoperative images of illustrative case
Five weeks post first stage of a surgically delayed pedicled transverse rectus abdominis musculocutaneous flap. (A) Frontal view and (B, C) profile views.
Two-year postoperative views of illustrative case
(A) Frontal view and (B, C) profile views. Note the good volume and shape match as well as the pliability and mobility of the reconstructed right breast, the latter as demonstrated by the right lateral diver’s view in (D).
DISCUSSION
Preoperative CT angiography in FFBR is useful as it illustrates donor vessels and abdominal wall vascular anatomy, allowing the surgeon to create a “road map” for surgery. However, our study has shown that a small number of cases can either prohibit surgery or impact the subsequent surgical plan due to previously undetected abnormalities. This underscores the utility of CTA as a preoperative tool. However, the financial and emotional costs associated with its use must be evaluated.
Our results show that over 10% of our patients had abnormal CT findings, which is similar to other reports in literature rates varying from 13% to 75% [12-14]. Although the primary objective of preoperative CTA is to visualize the relevant vasculature, abnormal vessel findings represented a minority of the detected anomalies with benign liver lesions being the most prevalent abnormalities observed. This is consistent with prior studies [14,15]. Compared the general population, patients with a breast malignancy have a similar prevalence of incidental findings but their findings are more likely to be of a severe nature [16]. This may be because the incidence of incidental findings on CTA is reportedly higher in women and patients aged over 40 years [16]; both of which are common characteristics of the breast cancer patient. Therefore, preoperative CT may also have an additional role in screening for incidental findings that may prove catastrophic if discovered in the operating theatre. Currently, there is a paucity of data detailing the incidence of incidental findings on abdominal CTA for other cancers. However, a comparison of the prevalence of incidental CTA discoveries between breast cancer and other malignancies is an interesting avenue for future investigation.
CT angiography has been shown to highly accurate with a 95% concordance rate between reports and operative findings [5]. CTA is, however, more expensive than other imaging modalities. The median approximate cost of a CT scan is £500, followed by magnetic resonance imaging (MRI) at £350, and ultrasound at £327. However, when evaluating DIEP flap vasculature, CTA is considered superior to other modalities, such as magnetic resonance angiography or color Doppler ultrasound. Yet, there is still risk of false positive results which can lead to additional unnecessary investigations. Earlier studies suggest that use of a preexisting CTA is an economical viable alternative to a fresh scan [17] which requires another radiation dose and further costs. However, nearly a fifth of our abnormal findings were significant enough to alter or cancel surgery. It is not possible to predict when these anomalies first become visible on CTA and using a preexisting CTA may result in missed diagnoses. It is clear that incidental findings on CT angiography can influence decision making in, and in some cases, preclude FFBR. Given the increased prevalence of severe abnormal CTA findings in the breast oncology population, we argue that the potential benefits of a preoperative CTA outweigh the risks in the breast cancer patient.
Furthermore, results from CTA can cause a change in operative plan [18]. Importantly, our results have demonstrated that discovery of incidental CTA abnormalities can prevent doomedto-fail or poor outcome flap surgery, as shown with the three patients whose “incidentalomas” prevented surgery. The emotional impact on the patient of having a failed reconstruction is not financially measurable but is emotionally devastating [19]. In addition, the cost saving implications of this can be considerable and it further strengthens the case for preoperative CTA evaluation in microvascular breast reconstruction. Flap failure, either partial or complete, is costly in a number of ways e.g. returns to theatre, prolonged hospital stays, repeat dressings and clinic attendances in addition to a future reconstruction [20]. It also emphasizes the importance of obtaining and reading the CTA report from an experienced radiologist.
In our study there were three patients that required additional imaging ranging from ultrasound to MRI. The outcome of that imaging did not affect the subsequent management plan in two-thirds of these patients. However, it could cause operative delay, anxiety to the patient while waiting for results, and the health economic cost of investigating asymptomatic patients is steep [21]. Delay in time to surgery is associated with increased mortality in breast cancer patients [22]. However, within our study patients with abnormal findings received surgery at a similar time interval to those without findings. This may reflect the urgency commonly employed in treatment of malignancies, whereby physicians fast track oncology patients to ensure timely care is given–this is called “cancer-pathway” priority. When the costs of subsequent investigation of incidental findings are taken into account, the cost of a preoperative CTA is estimated to be 30% greater than originally priced [23]. However, the potential rewards are immeasurable. Metastatic breast cancer was identified in one patient and this dramatically changed her prognosis and treatment plan. Future cost-benefit analysis is needed to determine the efficacy of these further investigations.
We acknowledge that this is a small cohort of patients and larger numbers are required to elucidate definitive trends. As breast cancer outcomes continue to improve, we will undoubtedly see a rise in absolute numbers of patients seeking primary reconstruction with abdominal based flaps as well as those who may have had prior implant-based surgery and are now seeking autologous tissue revisional surgery. With 10% of our patients having an unexpected finding on CTA, this could have potential ramifications for units such as ours which perform large volumes of abdominal based FFBRs.
This paper provides a quantitative overview of the prevalence and clinical outcomes of abnormal CTA findings but we would like to further study patient’s perspective. News of an incidental finding or abnormal medical test result can provoke feelings of stress and anxiety [24,25] and future qualitative studies may help guide how we influence the patient pathway when there is a possibility of unexpected findings and need further investigations.
CT angiography in breast reconstruction has a wider impact than facilitating surgery and reducing operative times. Incidental CTA findings can influence the surgical plan and avoid doomed-to-fail or poor outcome abdominal based free flap surgery in breast reconstruction, by detecting possible contraindications to surgery, such as absent DIE vessels or metastases.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication and the use of their images.
Author contribution
Conceptualization: Hamed RR, Oni G, Koo BC, Malata CM. Data curation: Ngaage LM, Ghorra DT, Ang J, Koo BC, Benyon SL, Irwin MS, Malata CM. Formal analysis: Ngaage LM, Koo BC, Malata CM. Writing original draft: Ngaage LM. Writing - review and editing: Ngaage LM, Hamed RR, Oni G, Ghorra DT, Ang J, Koo BC, Benyon SL, Irwin MS, Malata CM. Approval of manuscript: all authors.