Penetrating Trans-Orbital Injury from a Brush Handle Lodged in the Infra-Temporal Fossa
Article information
The infra-temporal fossa (ITF) contains major vessels and cranial nerves. It is divided into two regions: the retro-styloid region, which includes cranial nerves IX and XII, the jugular foramen, and the internal carotid artery; and the pre-styloid region, which includes the trigeminal and facial nerves [1]. The penetration of trans-orbital injuries is rarely observed in emergency departments, and there are few reports on intra-cranial involvement in such injuries. However, non-projectile penetrating ITF injuries due to foreign bodies are extremely rare [2].
We encountered a 24-year-old male who was admitted at our hospital with complaints of right eyeball pain, dizziness, and a foreign body in his right orbital area. His history revealed that he fell on a toilet brush after slipping in the toilet. On physical examination, the brush handle was observed to have entered the globe between the subtarsus and the infra-orbital rim, with minimal bleeding at the wound margins (Fig. 1). Mouth opening was limited. Although the patient was unable to open his right eye, forced lid elevation revealed mydriasis. The right globe was inferiorly fixed, and ocular movement was limited in all directions. The object pressed the globe. Although hypoesthesia was detected in the area of the infra-orbital nerve, no step deformity was detected on the orbital rim upon palpation. Visual acuity could not be evaluated because of the brush handle. A direct lateral graphic view and computerised tomography (CT) revealed a remarkable foreign body, 13 cm in length, lodged in the ITF and projecting into the floor of the right orbit. This caused a blowout fracture of the orbital floor of the right orbit and the posterior lateral wall of the maxillary sinus (Figs. 2, 3). Radiological images revealed no major vascular injury; however, the tip of the foreign body was close to the carotid canal and jugular fossa. ITF exposure may cause serious complications because of the foreign body's proximity to significant neurovascular structures. Because the object pressed the globe, we proceeded to the operating room for a simple procedure to withdraw the object immediately.

Photograph of the patient's eye upon entering the emergency room.
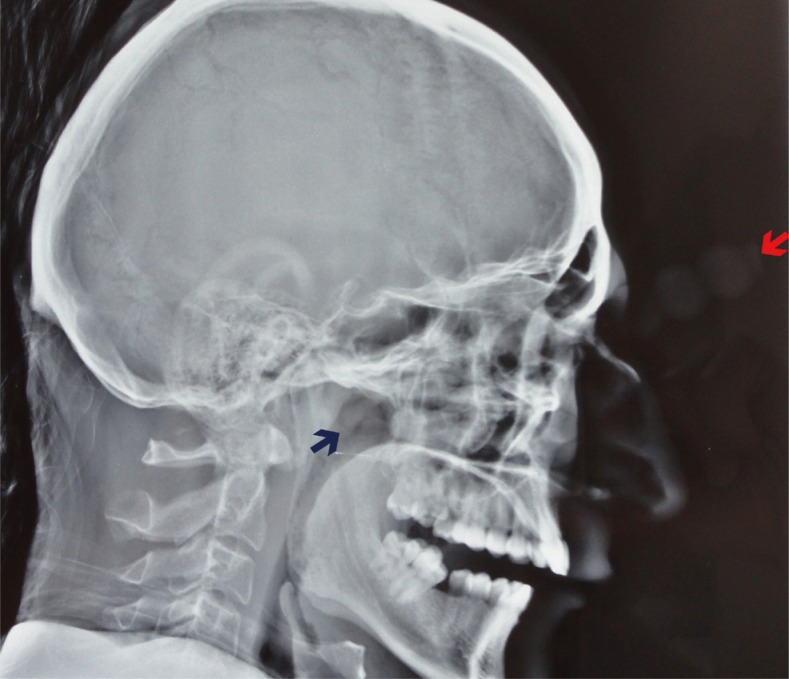
Head radiograph from lateral perspective; the red arrow indicates the head of the object, and the blue arrow indicates the end of the object.
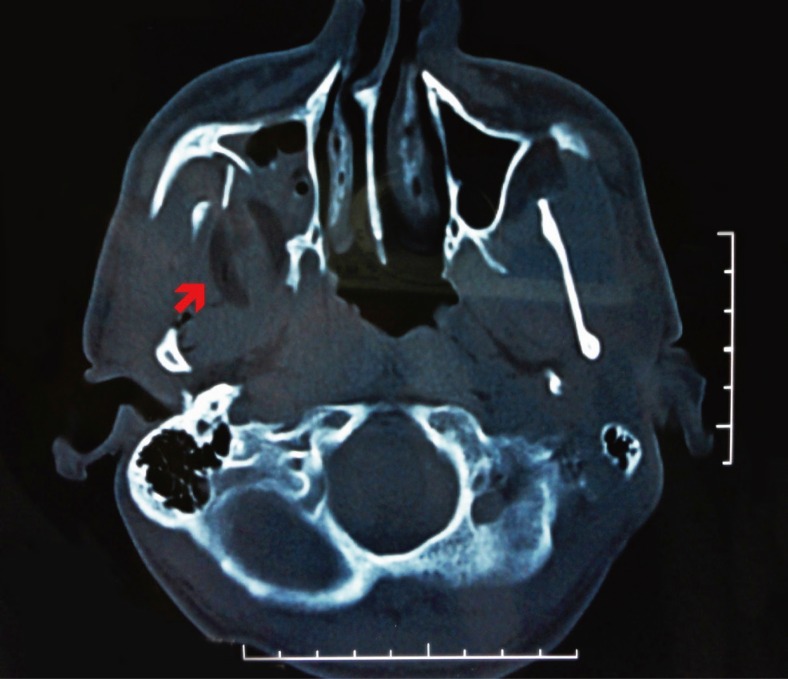
Computerised tomography (CT) image; the red arrow indicates the tip of the foreign body lodged in the infra-temporal fossa.
The outside handle of the object was cut off with an electronic saw to create a sterile environment. Subsequent gradual, simple intraoperative CT-guided withdrawal of the object did not cause any neurovascular damage. Endoscopy was used to help control bleeding through the wound. The globe was observed to be intact. The orbital floor was exposed through a subciliary incision; an approximately 4-cm2 defect was detected and repaired with a Medpor implant. Systemic and local antibiotic therapy (cefazolin 1 g, 3×1; tobramycin drops, 4×1) was started preoperatively and was continued until the wound healed completely. The patient recovered completely in 2 weeks. At the 6-month follow-up, the results were satisfactory; the control CT and magnetic resonance-angiography results were normal (Fig. 4).

Six months after the operation; the results were satisfactory.
In ITF injuries, the routes of entry are usually an injury through the maxillary region or the oro-antral region. Jagannathan et al. [2] reported a case of entry of a foreign body through the orbital floor, into the ITF through the posterior wall of the maxilla, without any injury to the conal structures. To the best of our knowledge, the current report is the second case describing this route. To explain this injury mechanism, we speculate that when a forceful blow is encountered in the upward direction, the impact is directly transmitted to the orbital floor without contacting the orbital rim or the globe. This occurred because the orbital floor forms an upward slope that is not parallel to the Frankfort horizontal plane, and the globe was saved because of the fluid malleability of the contents of the globe (Fig. 5).
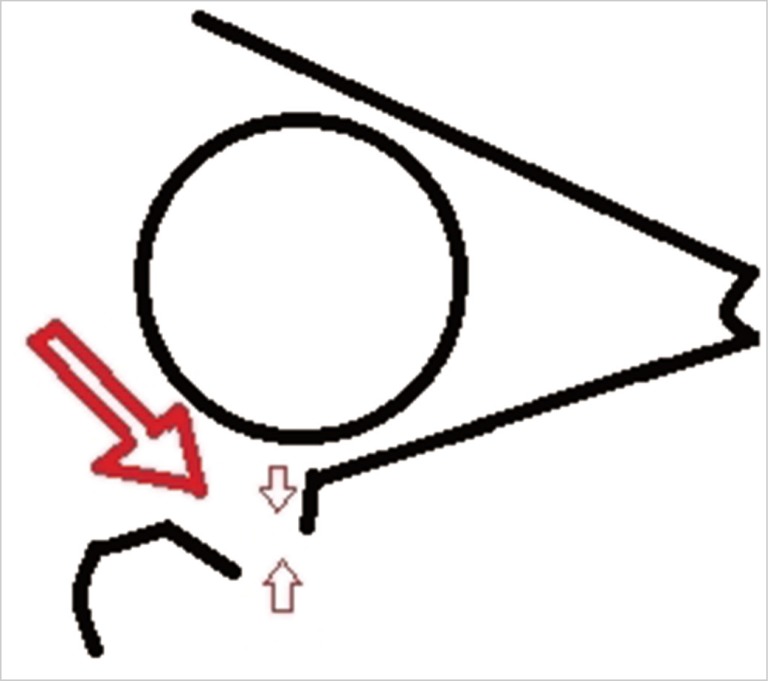
Schematic representing the mechanism of the blowout fracture: In infra-temporal fossa injuries, force is directly applied to the orbital floor without contacting the orbital rim or the globe, and an orbital floor fracture is produced. The big red arrow indicates the force direction and the small arrows indicates the locataion of fracture.
Access to the ITF is difficult. Traditional techniques include anterior (trans-facial) and lateral (pre-auricular and trans-temporal) approaches. The anterior approach presents a poor aesthetic outcome because it results in a large scar on the maxillary region. The lateral approach has a risk of damaging the facial nerve. Endoscopes allow surgeons to access the human body with relatively little surgical exposure, resulting in less tissue disruption. Endoscopic techniques decrease morbidity by decreasing surgical dissection [3].
It has been reported that simple withdrawal, performed in the operating room, causes no untoward effect [4]. However, a thrombotic carotid obstruction has been reported following the simple withdrawal of a foreign body from the ITF because of the external compression of the local hematoma and scar tissue formation [5]. Therefore, after a physical examination and radiological investigations, we decided that a careful intraoperative CT-guided withdrawal of the object and the use of an endoscope to control bleeding would be more reliable. The satisfactory result of this case supports the assertion that this line of management is appropriate in such injuries.
In this injury, the primary response is to perform preoperative steps (e.g., quick transportation to the hospital, radiological imaging, and patient elevation). In addition, an emergency operation should be planned considering the pressure on the globe and the optic nerve. In other kinds of blowout fractures and trans-orbital penetrating injuries, the operation is generally performed after the resolution of the edema. Otherwise, blindness is inevitable. In our case, we recognised this situation and achieved favourable outcomes. From our experience, we suggest that excellent visualisation by intra-operative CT before removing the foreign body along with attempts at bleeding control by an endoscope after the above-mentioned removal should be performed to avoid damage to the intra-orbital and ITF structures.
Knowledge of anatomic relationships at the ITF is critical in such injuries; emergency medicine physicians should not attempt to withdraw foreign bodies themselves but should consult maxillofacial surgeons. Trans-orbital penetrating injuries should be treated by using up-to-date technical developments such as endoscopy and intra-operative CT in order to increase safety. We believe that this is the most conservative and appropriate approach for such injuries.
Notes
This article was presented (as a poster) at the Turkish Association of Plastic Surgery Congress on 31st October-4th November, 2012 in Antalya, Turkey.
No potential conflict of interest relevant to this article was reported.