Congenital bilateral second metacarpophalangeal joint stiffness
Article information

Hand movement, especially in the fingers, is very important for quality of life [1]. In the fingers, the metacarpophalangeal joint (MCPJ) and proximal interphalangeal joint are more important functionally than the distal interphalangeal joint [2]. In this article, we report a rare case of a patient with congenital bilateral stiffness in the second MCPJ, inherited from the mother, that needed no surgery or intervention. This is the first reported case of congenital bilateral second MCPJ stiffness without any external trauma history.
A 30-year-old man visited the hospital because of finger stiffness. No visual abnormalities of his hand were noted, but the patient could not fully flex his second MCPJ actively (Table 1, Fig. 1).
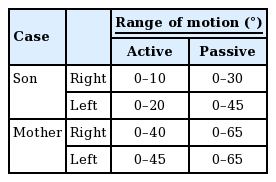
Range of motion of the second metacarpophalangeal joint in the mother and son
Images of both hands making a fist for the son (A) and mother (B). Both index fingers protruded more than the other fingers when making a fist on both sides.
Fig. 2 illustrates extrinsic tightness in both index fingers. The right side was more severely impacted than the left side.

(A, B) Extrinsic tightness test on the right second metacarpophalangeal joint (MCPJ). After the examiner pushed the patient’s index finger to flex the MCPJ in the proximal interphalangeal joint (PIPJ) and distal interphalangeal joint (DIPJ) flexed positions, the MCPJ could not be flexed without full extension of the PIPJ and DIPJ.
On an X-ray examination, ultrasonography, and magnetic resonance imaging, there were no abnormalities except for a bump on both second metacarpal heads on the X-ray examination and right MCPJ dorsal capsule contracture on ultrasonography. The mother’s X-rays also showed bumps on both second metacarpal heads (Fig. 3).
X-ray views (anteroposterior and oblique) of both hands for the son (A) and mother (B). It was noted that there were volar bumps of both second metacarpal heads. The yellow arrow shows the bony bump on the metacarpal heads.
Because of the long duration of the stiffness, the patient had to adjust his finger use, substituting his middle finger for his index finger in all motions due to stiffness in the second MCPJ. To increase the range of motion of the second MCPJ, corrective surgery may be needed. However, in some situations, surgery can worsen a patient’s functional status. In our opinion, the choice of whether to perform surgery in such cases should be made based on the patient's condition.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Keimyung University (IRB No. DSMC 2020-09-070) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained.
Patient consent
The patients provided written informed consent for the publication and the use of their images.