Facial injury patterns associated with stand-up electric scooters in unhelmeted riders
Article information

Abstract
Background
In recent years, the number of people riding stand-up electric scooters in South Korea has increased rapidly. This study analyzed the facial injury patterns associated with stand-up electric scooter-related trauma in patients who visited our emergency center.
Methods
In this retrospective review, we collected data from patients who had visited our emergency center for stand-up electric scooter-related trauma between January 1, 2018 and December 31, 2020.
Results
The average age of the patients was 26.7 years. Of the 73 patients, 47 were male and 26 were female, highlighting a male predominance. Seven patients were injured after alcohol consumption. None of the patients had worn helmets. Additionally, upon comparing the frequency of facial injuries according to the quarter of the year, the facial injury rate was higher in the second and third quarters than in the first and fourth quarters. Facial soft tissue injuries were classified into facial cosmetic subunits and analyzed according to their location. The highest number of injuries was on the chin (n=18, 20.9%). Of the 73 patients with stand-up electric scooter-related facial injuries, 16 had acute facial osseous fractures. The commonest acute facial osseous fractures were those of the orbit (n=7, 26.9%).
Conclusions
The patterns of facial trauma reported here can be helpful for quickly evaluating and treating patients with facial trauma related to stand-up electric scooters. Additionally, people riding stand-up electric scooters should be aware of the risks associated with facial trauma and the importance of wearing protective devices, such as helmets and masks.
INTRODUCTION
Stand-up electric scooters are environmentally advantageous in that they use electricity. They have recently been highlighted as a new means of transportation because they can be used conveniently in large cities. In recent years, the number of people riding stand-up electric scooters in South Korea has increased rapidly [1,2].
Several studies are being conducted globally on the injury patterns associated with stand-up electric scooter-related trauma. However, in South Korea, studies on these injury patterns have not been actively pursued because stand-up electric scooters were only introduced in South Korea relatively recently. Therefore, the purpose of this study was to analyze the facial injury patterns associated with stand-up electric scooter-related trauma in patients who visited our emergency center.
METHODS
The study was approved by the Institutional Review Board of Chung-Ang University Hospital (IRB No. 2104-006-19362). In this retrospective review, we collected the data of patients who had visited our emergency center for stand-up electric scooterrelated trauma between January 1, 2018 and December 31, 2020. Data were collected from the medical records of patients with stand-up electric scooter-related trauma. Only patients with facial trauma were included. If the injury was not directly associated with stand-up electric scooter-related trauma, such as a pedestrian being hit by a stand-up electric scooter, it was excluded from the analyses. In addition, none of the patients with injuries related to stand-up electric scooter use who visited our emergency center were wearing a helmet at the time of injury. Therefore, the data were analyzed only for unhelmeted riders.
The basic demographic information and baseline characteristics of patients with stand-up electric scooter-related facial trauma were analyzed using descriptive statistics. Data regarding soft tissue injuries and facial bone injuries caused by facial trauma were also analyzed.
Soft tissue injuries were classified as contusions, abrasions, and lacerations according to the degree of injury, and facial bone injuries were analyzed using facial three-dimensional computed tomography. Soft tissue injuries and facial bone injuries were classified and organized according to the region of injury and were projected on illustrations of the skull or face (Figs. 1, 2). Each soft tissue or bone injury was considered an individual injury, and the total number of each category of injuries was defined as the sum of individual injuries.
Illustrations of facial soft tissue injuries categorized by aesthetic subunit (scalp: 19.8%, forehead: 8.1%, eyebrows: 9.3%, eyelids: 5.8%, nose: 5.8%, cheeks: 14.0%, upper lip: 12.8%, lower lip: 2.3%, chin: 20.9%, ears: 1.2%).
Illustrations of bony injuries (skull: 0%, orbit: 26.9%, nasal bone: 19.2%, zygomatic bone: 19.2%, maxillary bone: 19.2%, mandible: 15.3%).
Data were entered into Excel 2013 (Microsoft Corp., Redmond, WA, USA).
RESULTS
Baseline characteristics
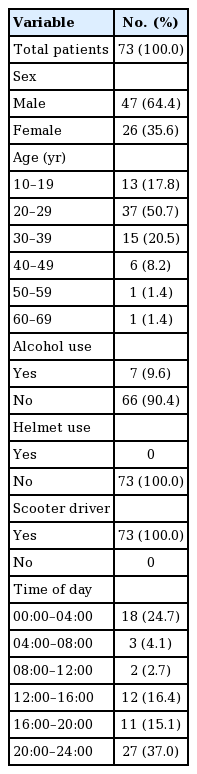
Between January 1, 2018 and December 31, 2020, 73 patients visited our emergency center after experiencing facial injuries associated with stand-up electric scooter-related trauma. All patients were riding stand-up electric scooters. The average age of patients was 26.7 years, and most patients were in their 20s. Of the 73 patients, 47 were male and 26 were female, highlighting a male predominance. Seven patients were injured after alcohol consumption. None of the patients had worn helmets (Table 1). As a result of the analysis according to the mechanism of facial injuries, seven patients had an accident that occurred after they collided with a car, and the remaining 68 patients fell by themselves while driving. The number of patients with facial injuries associated with stand-up electric scooter-related trauma increased significantly in 2020 compared to the previous 2 years. Additionally, a comparison of the frequency of facial injuries according to the quarter of the year showed that the facial injury rate was higher in the second and third quarters than in the first and fourth quarters (Fig. 3). An analysis of injuries according to the time of day when they occurred (in 4-hour intervals) showed that the highest number of patients was injured in the 20:00–24:00 period (27 patients; 37.0%), followed by 18 patients (24.7%) in the 00:00–04:00 period (Table 1).
Characteristics of patients
Number of facial trauma cases related to stand-up electric scooter use. Q, quarter.
Soft tissue injuries
Facial soft tissue injuries were classified into facial cosmetic subunits and analyzed according to their location, such as on the forehead, cheeks, eyelids, nose, chin, scalp, upper lip, lower lip, and ears [3]. The highest number of injuries was found on the chin (n = 18, 20.9%), followed by the scalp (n = 17, 19.8%) and cheeks (n = 12, 14.0%). Overall, 86 soft tissue injuries were analyzed; they included lacerations (n = 41, 47.7%), abrasions (n = 24, 27.9%), and contusions (n = 21, 24.4%) (Table 2, Fig. 3).
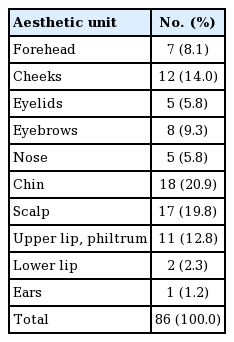
Classification of soft tissue injuries
Acute facial osseous fractures
Of the 73 patients with stand-up electric scooter-related facial injuries, 16 had acute facial osseous fracture; of them, six had at least two acute facial fractures. The commonest acute facial osseous fractures included those of the orbit (n = 7, 26.9%), followed by those of the nasal bones, zygomatic bones, and maxillary bones (n = 5, 19.2%). Among the patients with acute facial fractures, 10 patients (62.5%) underwent surgery and six patients (37.5%) underwent conservative treatment (Table 3, Fig. 1).
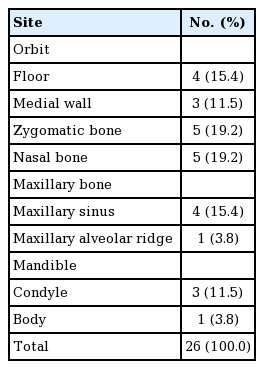
Classification of bone injuries
Neurological symptoms
Neurological symptoms such as loss of consciousness, seizures, headache, and nausea were present in seven of the 73 patients. All patients with neurological symptoms underwent brain computed tomography, and abnormal findings were found in three patients. One out of those three patients showed intracranial hemorrhage and subarachnoid hemorrhage; therefore, craniectomy and hematoma removal were performed. In the remaining two patients, traumatic subdural hemorrhage was confirmed and conservative management was performed.
DISCUSSION
In South Korea, the distribution of stand-up electric scooters began in Gangnam-gu in September 2018, and their use has gained nationwide popularity subsequently [4]. According to the Personal Mobility Alliance, the total number of trips using stand-up electric scooters in Korea from July 1 to December 15, 2019 exceeded three million [4]. Therefore, stand-up electric scooters are as popular as bicycles for personal transportation.
At the time of their introduction, stand-up electric scooters could be used by anyone over the age of 13 without a driver’s license. However, in recent years, the number of users of stand-up electric scooters has increased along with the number of related injuries. Therefore, the existing Road Traffic Act was amended to address these problems. Accordingly, on May 13, 2021, the minimum age for using stand-up electric scooters was revised from 13 years to 16 years. Additionally, only those with a valid driver’s license can ride these scooters, and safety equipment (e.g., hard helmets) must be worn. These changes are expected to be accompanied by a reduction in the incidence of facial injuries associated with stand-up electric scooter-related trauma and changes in facial injury patterns.
A previous study on facial soft tissue injuries associated with stand-up electric scooter-related trauma found that lacerations were the commonest injuries [5]. In accordance with these results, lacerations were the commonest soft tissue injury in this study as well (n = 41, 47.6%).
A previous study on bone injuries associated with stand-up electric scooter-related trauma found that orbital wall fractures were the commonest fractures, followed by fractures of the nasal bones and maxillary bones [6]. Similarly, in this study, orbital wall fractures were the commonest fractures, followed by bone injuries (nasal, zygomatic, and maxillary bones) of the mid-face area. A comparison of these findings with the previously reported patterns of bicycle-related facial bone injuries [7] shows that bicycle-related facial bone injuries differ from those of stand-up electric scooter-related bone injuries in that nasal bone injuries were commonest with bicycles.
In this study, an analysis of soft tissue injuries according to the injured area revealed that the highest number of injuries was on the chin (n = 18, 20.9%) [3]. However, bone injuries of the mandible were less common than those of the orbit, nasal bones, maxillary bones, and zygomatic bones.
The lower face injuries associated with a stand-up electric scooter involved relatively low-energy trauma. Similarly, the frequency of soft tissue injuries in the forehead area was high, whereas bone injuries of the frontal bone were not observed; therefore, the forehead also received relatively low-energy trauma.
In this study, most of the bone injuries occurred in the midface area (nasal, maxillary, orbital, and zygomatic bones). Therefore, facial bone injuries associated with stand-up electric scooter-related trauma are the commonest in the mid-face area. These results are similar to the patterns of facial trauma in road cyclists [8].
Seventeen soft tissue injuries, which accounted for 19.8% of the soft tissue injuries, were noted in the scalp area (Table 2). Considering that none of the patients in this study were wearing a helmet, it would be reasonable to expect that the adoption of helmet use would reduce the considerable number of facial injuries in the scalp area [9]. In addition, neurological symptoms such as loss of consciousness, seizures, headache, and nausea were present in seven patients in this study. Three of them suffered severe brain damage (e.g., intracranial hemorrhage, subarachnoid hemorrhage, and subdural hemorrhage). It is hoped that wearing helmets will reduce the risk of traumatic brain damage associated with stand-up electric scooter use [9]. In the future, this study is expected to serve as a legal basis supporting the law that a helmet must be worn when riding a stand-up electric scooter. The limitations of this study are that the risk factors (e.g., velocity, location, and time) of facial injuries were not analyzed and that the study was conducted at a single institution. Further studies are needed to overcome these limitations. Additionally, if studies on the costs involved in the event of facial trauma related to stand-up electric scooter use are conducted in the future, we believe that they will be helpful to the riders of these scooters.
The patterns of facial trauma reported here can be helpful for quickly evaluating and treating patients with facial trauma related to stand-up electric scooters. Additionally, people riding stand-up electric scooters should be aware of the risks associated with facial trauma and the importance of wearing protective devices, such as helmets and masks.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Chung-Ang University Hospital (IRB No. 2104-006-19362) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived because this study design is a retrospective chart review.
Author contribution
Conceptualization: TH Bae. Data curation: WS Kim, HK Kim, SH Kang. Formal analysis: HS Kim, WS Kim, HK Kim, SH Kang. Methodology: WS Kim, HK Kim, SH Kang. Writing - original draft: HS Kim. Writing - review & editing: TH Bae.