Pilomatricoma Arising at an Influenza Vaccination Site
Article information
Pilomatricoma is a benign skin neoplasm that arises from hair follicle matrix cells. It occurs on the head, neck, and upper extremities, and less frequently on the trunk and lower extremities. The etiology of pilomatricoma is subject to controversy. Trauma, insect bites, or surgery are thought to be antecedent events to the onset of the tumors. Influenza vaccination is a common annual event among individuals. Complications are usually mild and self-limiting. Prophylactic influenza vaccinations rarely cause cutaneous complications. Few cases of foreign body granuloma, infectious reaction, and other cutaneous complications have been reported. In this article, we describe a case of pilomatricoma arising at an influenza vaccination site. Although there has been a report of an association between pilomatricoma and bacille Calmette-Guerin (BCG) vaccination [1], an association with influenza vaccination has not been reported previously. The clinical manifestations and progress of the case are presented in this report. A 7-year-old girl received her routine influenza vaccination in the left upper arm. One month later, a sensation of warmth and redness developed on the vaccination site. Serous discharge was drained with a small amount of blood. Three months later, the patient was referred to the plastic surgery outpatient department, where she presented with a pinkish ulcerative nodule on her left upper arm at the site of administration of the influenza vaccine. At that time, the nodule was covered with a dressing, but it gradually became harder to the touch and larger in size.
Seven months later, the nodule reached approximately 10 mm in diameter, and was fixed firmly to deep subcutaneous tissue (Fig. 1). Ultrasonographic examination revealed a heterogeneous echo texture, surrounding subcutaneous fat infiltration, and subtle vascularity (Fig. 2). Clinical differential diagnoses included foreign body granuloma, postvaccinal lymphadenitis, and pilomatricoma.

Nodule connected to the subcutaneous mass, at the site of administration of the influenza vaccine.
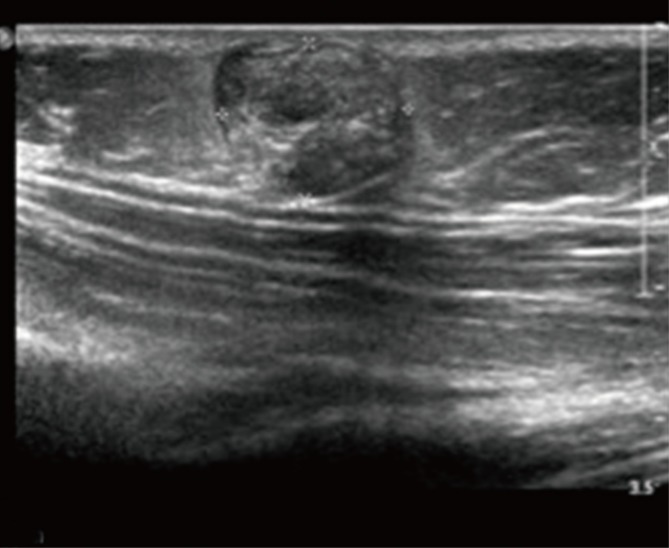
Heterogeneous mass-like lesion, 15 mm in diameter, embedded in subcutaneous layer.
An excisional biopsy was performed. The nodule and embedded mass-like lesion were completely removed. Grossly, the specimen was surrounded by inflammation tissue (Fig. 3). Microscopic examination revealed a well-demarcated lesion stemming from the dermis that consisted of multinucleated giant cells and ghost cells with a central unstained area indicative of a lost nucleus. The characteristic basaloid cells were also identified. These cells were surrounded by a lining of squamous cells (Fig. 4). The specimen was identified as a completely excised pilomatricoma, with clear margins. There was no local recurrence at the patient's follow-up visit 7 months later.

Gross specimen containing projecting nodule and subcutaneous embedded mass-like lesion.
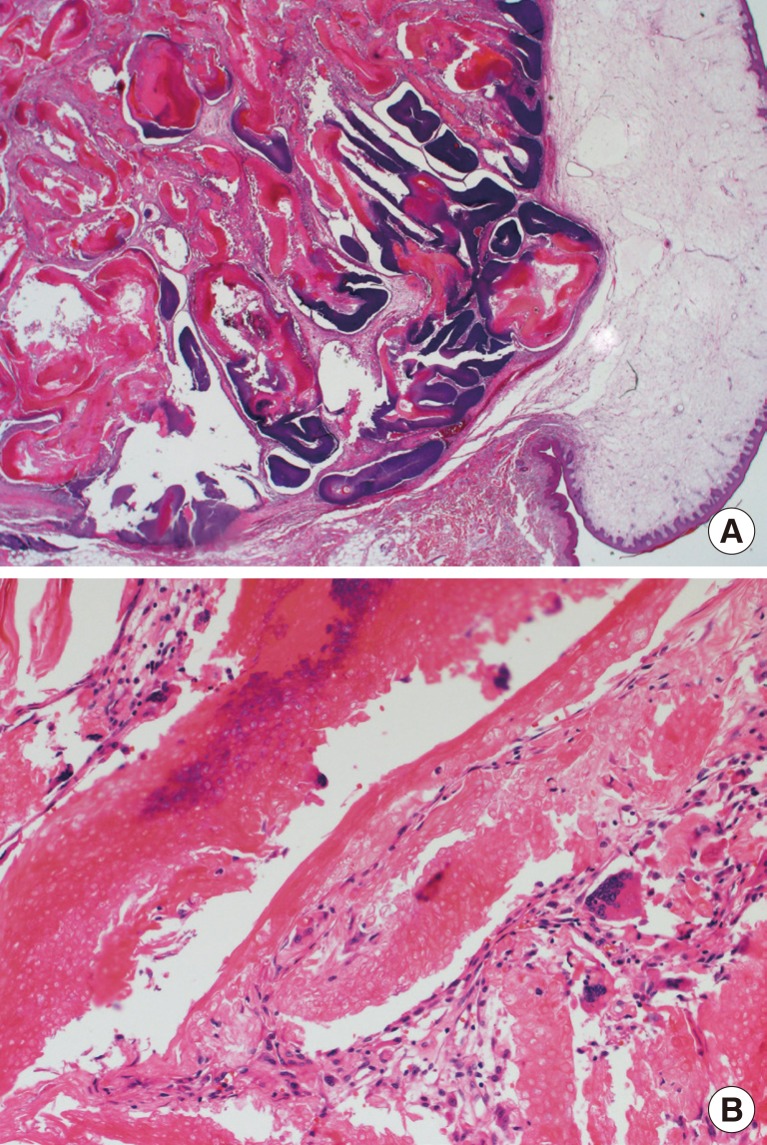
(A) Characteristic basaloid cells and squamous cell lining (H&E, ×12.5). (B) Cells without a detectable nucleus (ghost cells) and multinucleated giant cell at the periphery (H&E, ×100).
Pilomatricoma, also known as calcifying epithelioma of Malherbe, is a benign calcifying tumor that arises from the hair matrix and presents as a slow-growing dermal or subcutaneous mass. Duflo et al. [2] reported a 20% incidence of pain and inflammation associated with pilomatricoma.
Histologically, a pilomatricoma presents as a well-demarcated lesion, stemming from the dermis and extending into the subcutaneous fat. These lesions usually consist of islands of epithelial cells comprising basophilic cells with meager cytoplasm and ghost cells that have a central unstained area indicative of a lost nucleus. Although the etiopathogenesis is unknown, the virus and genetic mutation have been reported to be associated with the development of pilomatricoma [3].
Complete surgical excision remains the treatment of choice for benign pilomatricomas. In cases with tumor adherence to the dermis, the overlying skin might be excised. Although recurrence after complete excision is rare, recurrence rates of 2% to 6% were reported in the literature.
Tumors found in vaccination scars could be induced by trauma, persistent inflammation/wound healing, scarring, and/or the inoculated attenuated agent itself. Pirouzmanesh et al. [3] reported that inflammation was present in 40.8% of pilomatricomas in microscopic examinations. In our case, preceding inflammation was thought to be responsible for the pilomatricoma. Several adjuvant contained in vaccine have been found to produce more inflammation. Also, a needlestick injury or similar trauma causing damaged follicular epithelium at the injection site may lead to a faulty suppression of apoptosis which in turn, may result into the formation of pilomatricoma [4]. Hematoma after the injection may be followed by a rapidly growing pilomatricoma. Although exact pathologic sequence of the disease could not be defined, such prior events were though to be possible multifactorial causes. To our knowledge, pilomatricoma has not been reported to arise in scars or following an influenza vaccination, but one study reported an occurrence of the tumor following BCG vaccination [1].
Pilomatricoma is still frequently misdiagnosed. One study showed that the rate of preoperative diagnostic accuracy is less than 49% [3]. Pilomatricoma is difficult to diagnose because of its variant morphology and sometimes unusual appearance that may be similar to more common lesions. Furthermore, because vaccination is a relatively rare cause of pilomatricoma, differential diagnosis could be more difficult in this type of case. Therefore, histopathologic examinations are required for the final diagnosis. Basaloid cells and ghost cells are known to be the two key components for the diagnosis and sufficient for a confident pathologic diagnosis of pilomatricoma. The presence of foreign body-type cells, nucleated squamous cells, and calcification, alone or in combination, was less specific, but supported a diagnosis of pilomatricoma [5]. Influenza vaccination is widely performed. Cutaneous complications have been reported following influenza vaccination. Rash, pruritus and urticaria can be occurred as an minor complication. Despite cutaneous neoplasm due to influenza vaccine are not frequently reported, few cases have been reported. The pathogenesis of pilomatricoma following vaccination injection is intriguing. However, the exact pathogenesis in our case remains unexplored. Despite the uncertainty of the diagnosis, we suggest that pilomatricoma be included in the differential diagnoses of chronic nodular lesions arising at influenza vaccination sites.
Notes
No potential conflict of interest relevant to this article was reported.