Bipartite os Centrale Carpi in a Patient with the First Metacarpal Bone Fracture
Article information
The os centrale carpi is a relatively rare accessory carpal bone. It is located in the carpus among the capitate, a scaphoid, and trapezoid bones. This rare anomaly is believed to represent a remnant of a separate ossification center present in the human embryo at 6 weeks of gestation that normally fuses with the scaphoid. It seem to occur as isolated anatomic variants with an incidence of 0.3 to 1.6 percent [1]. This report describes a case of a bipartite os centrale carpi in a patient who was hospitalized for a fracture of his first metacarpal bone, separately presenting as focal tenderness of the wrist and dorsoradial area. A 15-year-old male was hospitalized for painful swelling on his left hand after falling. He was diagnosed with a first metacarpal bone fracture based on plain radiographic imaging. Coincidentally, small triangular bony fragments were seen at the distal medial end of the scaphoid on the same radiograph. The margins of this fragment were smooth, presenting a normal density but a vague double contour (Fig. 1). Upon clinical examination, range of motion and grip strength were normal, no swelling was seen, but palpation tenderness was present over the dorsoradial part of his right wrist. computed tomography (CT) images demonstrated 2 pieces of smooth triangular ossicles in the dorsal aspect of the joint among the scaphoid, a capitate, and trapezoid bones. These ossicles, which are referred as 'os centrale carpi', were found to be two separated fragments (Fig. 2). The plain radiograph didn't show any evidence of ossicles on the opposite wrist. Additional studies for the opposite wrist (three-dimensional [3D] CT) were suggested, but the patient refused. He was not aware of having developmental anomaly, with no history of congenital abnormality syndromes or of any preceding trauma. An operation was performed under general anesthesia using standard techniques. His left first metacarpal bone fracture was fixed with K-wire. Due to unrelenting symptoms, surgical excision of the ossicles was performed. We approached the fracture using a 0.02 m incision on the dorsal side of the wrist, which corresponded to the location of the fracture in the CT findings. Intraoperative findings revealed two pieces of mobile ossicles, each 0.005 m in diameter, among the capitate, the trapezoid, and the distal ulnar pole of the scaphoid. We also found small central cores of each ossicle, covered with a smooth cartilage surface and detached from the joint capsule (Fig. 3). At the last visit 5 months after the operation, the patient reported complete relief of focal tenderness of his wrist. Repeated examination of the postoperative CT findings did not show any sign of the removed accessory bone. The os centrale carpi, difficulties with diagnosis and pain due to the presence of ossicles have been seldom reported. Adolfsson [2] reported a case with intermittent wrist pain. The ossicles were mobile within the wrist and caused pain following movement of the surrounding carpal bones. Sacks [3] in 1949, described a similar case in which wrist pain was associated with mobile os centrale carpi. Arthroscopy was sufficient for diagnosis of the mobility of the ossicles and their simultaneous removal. The ossicles were mobile within the wrist and caused symptoms as a result of interference with movement of the surrounding carpal bones. Lane et al. [4] reported a case of a painful wrist due to osteonecrosis of an os centrale carpi and secondary degenerative changes. The cause of the osteonecrosis was trauma. The ossicle was partially attached to the scaphoid; this union was broken by the trauma. As the blood supply from the scaphoid was interrupted, the os centrale underwent avascular necrosis. This finding of os central carpi is a rare event; it may be misinterpreted as a fracture or overlooked on radiographs due to overlap of adjacent bones. This anomaly can be differentiated from soft tissue calcifications and other acute fractures, old nonunion fractures, avascular necrosis, bipartite scaphoid etc. An acute scaphoid fracture shows non-corticated sharp or irregular margins. An old scaphoid fracture may show a cyst-like formation or a pronounced patchy decalcification along the fracture line, which may represent osteopenia in the distal fragment [5]. There were 4 reasons to conclude bipartite os central carpi differentiate with other possibilities. Because the problems apparently began after a traumatic episode, it appears possible that the ossicles tore loose by a forced, sudden movement of the wrist (Fig. 4).

Initial plain radiograph. A first metacarpal bone fracture and small triangular bony fragments (red circle) at the distal medial end of the scaphoid were evident.

Preoperative three-dimensional computed tomography findings. Two pieces of smooth triangular ossicles (red circle) in the dorsal aspect of the joint among the scaphoid, capitate, and trapezoid bones were evident.

Intraoperative findings. Mobile ossicles were found to be separated into two pieces (red circle), each approximately 0.005 m in diameter, covered with smooth cartilage surfaces and detached from the joint capsule.
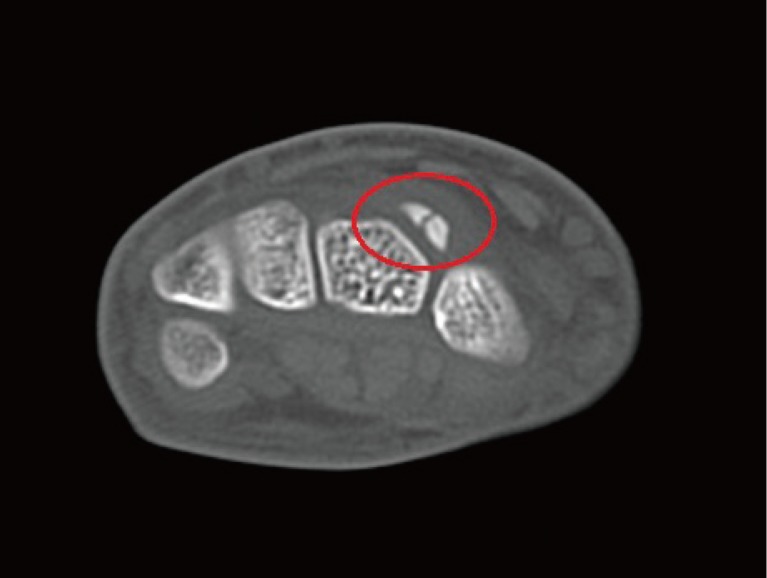
Preoperative computed tomography findings, axial view. The ossicles were made of an outer cortex and an inner medulla (red circle). Difference in density allows for differentiation on imaging finding, cortex being denser and therefore whiter. Inner medulla is surrounded by outer cortex, smoothly continuing the surface. And there was no evidence of cortical disruption or irregularity of other carpal bones.
First, the ossicles were made of an outer cortex and an inner medulla. Difference in density allows for differentiation on imaging finding, cortex being denser and therefore whiter.
Inner medulla is surrounded by outer cortex, smoothly continuing characteristics.
Second, there was no evidence of cortical disruption or irregularity of other carpal bones. So, we could conclude the fragments to be independent ossicles and rule out the fracture segments from scaphoid or etc.
Third, the ossicle showed round and smooth medulla and cortical bone except cortical disruption or any shrinked portion, sclerotic area, deferentiate from other diagnosis, especially osteonecrosis.
Fourth, surgical findings confirmed the diagnosis, showed mobile ossicles separated into two pieces, approximately 0.005 m in diameter each, covered with smooth cartilage surfaces and detached from the joint capsule. Each had a small central core, which is medulla portion. Removal of the ossicles resulted in symptom relief. This was rare case of a bipartite os centrale carpi emerging symptoms.
Notes
No potential conflict of interest relevant to this article was reported.