Cutaneous T-Cell Lymphoma with Nasal Necrosis
Article information
Mycosis fungoides is a rare T-cell cutaneous lymphoma that poses a unique diagnostic challenge given its heterogeneous presentation. The refractory case presented here highlights the need for advances in early diagnostic technologies.
A 73-year-old diabetic man presented with erythema and necrosis of the nose. He initially had a 7 mm squamous cell carcinoma on the nose which was excised with Mohs surgery. The wound rapidly progressed to full thickness necrosis of the left nasal ala without pain or fever. During subsequent reconstruction with a nasolabial flap and cartilage graft, biopsies of the nasal margin showed severe inflammation without malignancy. The reconstructed area failed to heal and serial cultures grew multiple species of bacteria which were treated with several courses of antibiotics. Erythema of the nose and face continued to progress over 7 months and new lesions appeared, including skin necrosis at the site of previous left ala flap, right dorsum of nose and right cheek (Fig. 1). Computed tomography (CT) scan showed no involvement of sinuses or facial bones. Repeat biopsy showed acute and chronic inflammation with no malignancy and no organisms. A few weeks later a new erythematous plaque developed on the back (Fig. 2) and biopsy showed lymphocytic infiltrate with a monoclonal T-cell population (Figs. 3, 4). Repeat assay of previous nasal biopsy showed the same T-cell receptor gene rearrangement leading to the diagnosis of cutaneous T-cell lymphoma, consistent with mycosis fungoides (MF). The patient was staged with positron emission tomography-CT scan showing no visceral disease despite developing new lesions in his groin in addition to new lesions on his back and face. He was treated with a combination of systemic chemotherapy, radiation and phototherapy. At 16 month follow up he has persistent skin lesions, with progression of tumor burden.

Facial involvement of mycosis fungoides with significant nasal necrosis at site of previous nasolabial flap.

Erythematous plaque distant to original lesion with biopsy results demonstrating cutaneous T cell lymphoma.
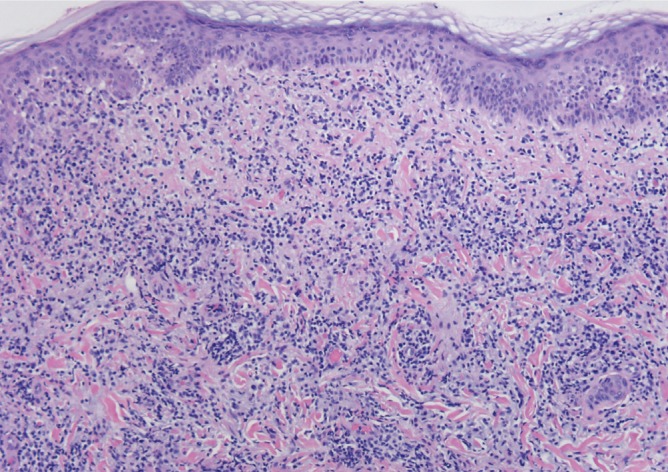
Diffuse lymphocytic infiltrate through the dermis with inconspicuous epidermotropism (H&E, ×6.3).
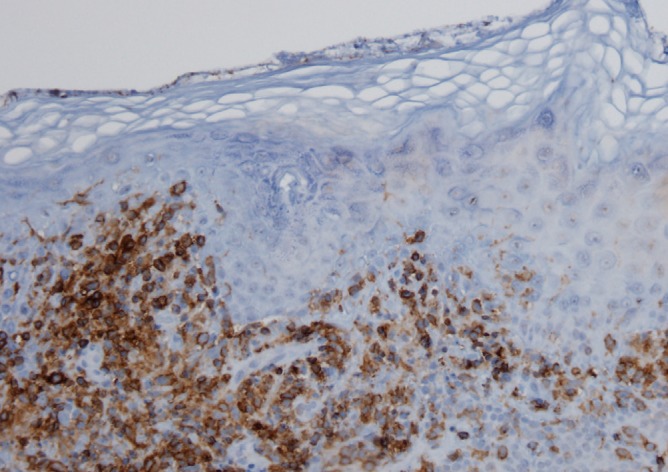
Immunohistochemical study demonstrates a predominance of lymphocytic cells labeling with CD4 with some extension into the epidermis (×12.6).
This case highlights the diagnostic difficulty seen in many cases of cutaneous T-cell lymphoma described in the literature. The diagnosis of cutaneous T-cell lymphomas, the majority of which are classified as Mycosis fungoides or Sezary syndrome, requires integration of both clinical and histopathological information [1]. The diagnosis of early MF is often difficult given its heterogeneous clinical and pathologic presentations [2,3]. Histopathologically, early MF may resemble chronic inflammatory dermatoses with reactive T cells and other immune cells [2,4]. Adjuvant techniques such as immunophenotyping and T cell receptor gene rearrangement studies can help make the diagnosis in some difficult cases [3]. The classic histopathology of MF is characterized by lymphocytes with cerebriform nuclei and a haloed appearance that display epidermotropism or populate the dermoepidermal junction [2,4]. Histological diagnosis of early disease typically requires several follow up skin biopsies [3]. Given the difficulty of diagnosis, clinic-pathologic correlation is crucial for early MF diagnosis [3], though the use of novel immunohistochemical and molecular biology techniques has been discussed as a method of helping with diagnosis [4]. Classic presentation of MF includes patches and plaques on non-sun exposed areas that may slowly evolve [2]. The patient's atypical clinical presentation likely contributed to the difficulty with diagnosis.
Treatment goals are typically determined by extent of disease, prognostic factors, quality of life, and patient comorbidities [5]. Staging is determined by skin, lymph node, viscera and blood involvement; in early disease, prognosis is generally favorable [5]. Therapy for early disease often includes topical corticosteroids, topical nitrogen mustard and phototherapy, total skin electron beam therapy and/or low-dose local radiation [5]. Systemic therapy is used in advanced cases or cases refractory to topical therapy. Interferons and retinoids are commonly used first-line, with histone deacetylase inhibitors, alemtuzumab also possible therapeutic agents. Chemotherapy is generally reserved for treatment refractory or rapidly progressive disease [5]. In this patient, chemotherapy was appropriate given his treatment refractory disease, with appropriate alterations in treatment after toxicities developed.
Notes
No potential conflict of interest relevant to this article was reported.