A Simple, Reliable, and Inexpensive Method for Seroma Drainage
Article information
Seromas and hematomas are relatively common complications of a variety of surgical procedures. In plastic surgery, they may occur in the postoperative period of abdominoplasty or abdominal wall reconstruction, mastectomy or breast reconstruction, lymphadenectomy, or voluminous neoplasm excision. Furthermore, in our experience, seromas are particularly common in surgical procedures involving the use of biological substitutes [1].
Clinical treatment of seromas is usually performed by repeated evacuation by means of suction using an appropriately sized syringe (usually 10-50 mL in volume) according to the amount of fluid to be evacuated [2]. In some cases, an ultrasound examination can highlight the depth, volume, and extension of the fluid. In the case of seromas that are more than 100 mL in volume, the use of several syringes is necessary. Whenever a syringe is filled, it should be replaced or depleted by unplugging it from the hypodermic needle, thus exposing the patient to a high risk of infection. Therefore, negative pressure cannot be maintained continuously [3]. In order to avoid these issues, we have developed a new and simple method that allows us to reduce the material used and to minimize the risk of infection.
This device involves the use of basic materials that are easily available in every hospital: a hypodermic needle, preferably a 20 G syringe needle, and high-vacuum Redon drainage. For this system, we used a high-vacuum Redon bottle (Drainobag 300V Lock, B-Braun, Melsungen AG, Germany); however, any kind of drainage can be used. First, it is necessary to make an oblique incision in the terminal portion of the rubber connector, taking care not to excessively shape the rubber in order to maintain the negative pressure. It is now sufficient to plug the connector into the needle hub to achieve the drainage system (Figs. 1, 2). Usually, an accurate plug between the needle and the connector is sufficient to maintain the negative pressure. To avoid disconnections, due, for example, to the stretching of the drainage tube, a plaster may be added to the connection.
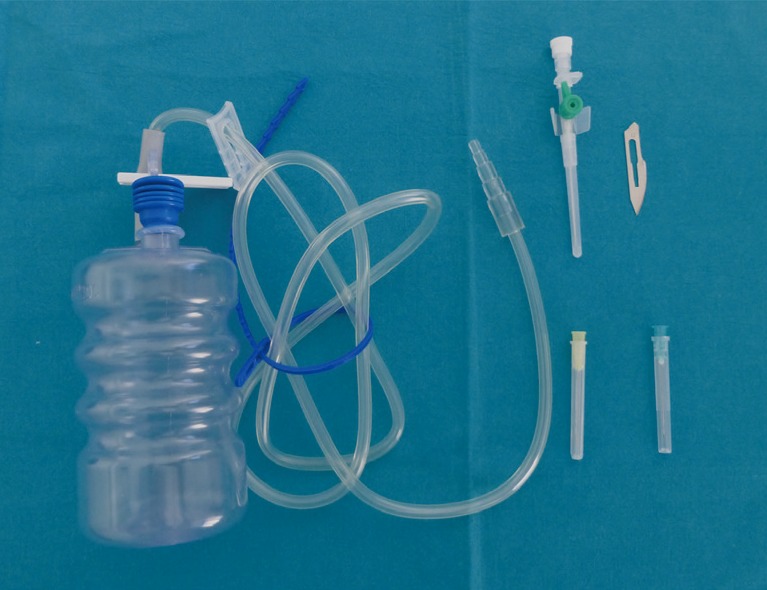
Equipment for seroma drainage system: a 20 G hypodermic needle (alternatively a 21 G hypodermic needle or a needle cannula), high-vacuum Redon drainage, and a blade.

The assembled seroma drainage system. In the box, the system with the cannula needle.
After pricking the skin and identifying the seroma, it is possible to open the drainage. The liquid will be drained from the drainage system without the use of different syringes. If a change of the drain site is necessary, simply close the Redon, prick the skin in another site, and reopen the drainage. It will suck the liquid without losing the negative pressure.
This simple technique offers many advantages such as the availability of the required materials, lower risk of infection due to absence of material changing, a reduction in the risk of losing seromas (possible during the syringe changes), easier handling of the needle as compared to the whole syringe, a reduced number of devices with a decrease in costs, and higher accuracy of the drained fluid volume quantification.
This easy drainage method can be used daily for both seromas and liquid hematomas. It is also possible to connect a cannula needle [4] as an alternative to the simple needle. This can be attached to the skin appropriately in order to obtain permanent aspiration. This technique appears to be more accurate and cheaper than traditional drainage methods and can be an excellent alternative in voluminous seroma drains.
Notes
No potential conflict of interest relevant to this article was reported.