Outcome Analysis of Cranial Molding Therapy in Nonsynostotic Plagiocephaly
Article information
Abstract
Background
It is known that nonsynostotic plagiocephaly does not spontaneously improve, and the craniofacial deformities that result from it. This study was conducted to analyze the effectiveness of helmet therapy for the nonsynostotic plagiocephaly patient, and to suggest a new treatment strategy based on this analysis.
Methods
A total of 108 pediatric patients who had undergone helmet therapy after being diagnosed with nonsynostotic plagiocephaly were included in this study. The patients were classified according to the initiation age of the helmet therapy, severity, and helmet wearing time. The treatment effect was compared using cranial vault asymmetry (CVA) and the cranial vault asymmetry index (CVAI), which were obtained from diagonal measurements before and after therapy.
Results
The discrepancy of CVA and CVAI of all the patients significantly decreased after helmet therapy. According to the initiation time of helmet therapy, the treatment effect was best at 5 months old or less. The helmet wearing time per day was proportional to the treatment effect up to 20 hours. In addition, the rate of the successful treatment (final CVA ≤5 mm) significantly decreased when the initiation age was 9.1 months or older and the treatment period was less than 7.83 months.
Conclusions
This study showed the effectiveness of the helmet therapy for nonsynostotic plagiocephaly patients. Based on analysis of this study, helmet therapy should be started at the age of 9 months or younger for 7.83 months or more, and the helmet wearing time should be more than 20 hours a day.
INTRODUCTION
Generally, nonsynostotic plagiocephaly is an asymmetrical condition of the head caused by an extrinsic factor such as molding rather than by an intrinsic factor such as craniosynostosis [1]. Nonsynostotic plagiocephaly is also called deformational plagiocephaly, positional plagiocephaly, or the flat head syndrome [2].
The causes of nonsynostotic plagiocephaly can be divided into prenatal and postnatal causes. The prenatal causes include uterine compression and intra-uterine constraint, and the postnatal causes include the sleeping position and congenital muscular torticollis. Among the causes of nonsynostotic craniosynostosis, sleeping position may be assumed to play a major role in the incidence of this condition. A study reported that the incidence of nonsynostotic plagiocephaly in the U.S. has dramatically increased since the implementation of the "Back to sleep" campaign, one of the regimens suggested by the American Academy of Pediatrics for preventing the sudden infant death syndrome [3].
Many studies have reported that nonsynostotic plagiocephaly does not spontaneously improve [4,5] and the craniofacial deformities such as asymmetry of the face and ear position, which result fron it, will also be permanent [6-11]. The asymmetric head caused by nonsynostotic plagiocephaly will worsen over time because the pediatric patient is usually positioned on the flattened area of the head in a supine position. Moreover, because its incidence rate is reported to be 1 in 300 newborn babies [12], the need for appropriate treatment for nonsynostotic plagiocephaly is becoming widely recognized. Treatment options for nonsynostotic plagiocephaly include head repositioning, helmet therapy, and surgery [13]. Among these, helmet therapy is most widely used. It can achieve treatment effects by inducing prominent areas to be retained passively and flattened areas to grow rapidly into the hollow space in the orthotic device [14]. Studies have reported that helmet therapy achieved about 3 times faster and better correction than head positioning alone [1,2,6,10,15]. However, no studies have reported on the effectiveness of helmet therapy in Asian or particularly Korean children because helmet therapy is not widely performed. Thus this study was conducted to analyze the effectiveness of helmet therapy for nonsynostotic plagiocephaly patients in the Republic of Korea.
METHODS
A total of 108 pediatric patients who had completed helmet therapy after being diagnosed with nonsynostotic plagiocephaly between 2008 and 2011 were included in this study. Of these 108 patients, 75 were male (69.4%) and 33, female (30.6%). A three-dimensional (3D) computed tomography (CT) scan of each patient confirmed that craniosynostosis was not present. The helmet was customized individually according to a 3D CT scan and the measurements of the patient's head including the anteroposterior, bitemporal, and diagonal distances using a spreading caliper, and the circumference using a tapeline (Fig. 1). Treatment effects can be achieved by inducing prominent areas to be retained passively and flattened areas to grow rapidly into the hollow space in the helmet [14]. According to the helmet therapy protocol of the authors' hospital, if the difference between each diagonal distance was more than 10 mm, helmet therapy was strongly recommended. When a patient's parents decided to undergo helmet therapy, the patients were followed up at 4- to 8-week intervals based on their ages and conditions. Three physicians measured the anteroposterior, bitemporal, and diagonal distances of the patient's head using a spreading caliper and head circumference using a tapeline. The measurements from three physicians were averaged before entering the doctor's office on every follow-up visit. The patient's parents were supposed to record the helmet wearing time everyday, and bring this form to the outpatient clinic.
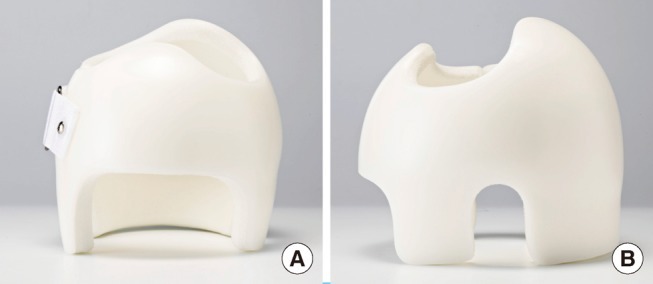
Helmet for cranial molding therapy
The helmet was customized individually according to a 3D CT scan and the measurements of the patient's head including anteroposterior, bitemporal, and diagonal distances using a spreading caliper, and circumference using a tapeline. The helmet can achieve treatment effects by inducing prominent areas to be retained passively and flattened areas to grow rapidly into the hollow space in the helmet. (A) The front, (B) the side of helmet.
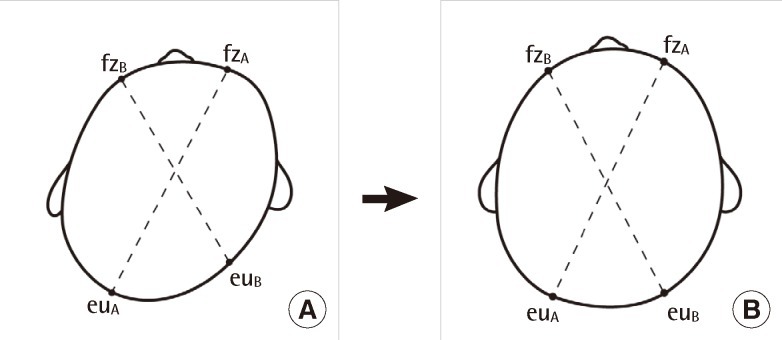
In each patient, the frontozygomatic-to-contralateral occipital (euryon) distance was measured on both sides using a spreading caliper. The distances were defined as diagonal A or B (A>B), and the cranial vault asymmetry (CVA) (diagonal A -diagonal B) and cranial vault asymmetry index (CVAI) ([diagonal A to diagonal B]/[diagonal A×100]) [14] were measured. Then the measured CVA and CVAI were compared with the initial measurements to assess the treatment effect and determine the termination of the therapy (Fig. 2). The patients were classified into group 1 (5 months or less, n=20), group 2 (6 to 8 months, n=38), group 3 (9 to 11 months, n=31), and group 4 (12 months, n=19), based on their initiation age of the helmet therapy (Table 1). In addition, the severity of the head asymmetry was classified into mild (6 to 10 mm, n=15), moderate (11 to 15 mm, n=34), and severe (≥16 mm, n=59) based on the initial CVA (Table 2). The compliance of the patients was classified into poor (<15 hours, n=24), good (15 to 19 hours, n=55), and excellent (≥20 hours, n=29), based on helmet wearing time in a day, which was obtained from the form that was filled out by the patient's parents (Table 3). The treatment termination was decided on by the physician based on the change in the CVA that was measured during the helmet therapy, the tolerance of the patients, and the satisfaction of the patients' parents. The data analysis was performed using PASW Statistics ver. 18.0 (IBM Co., Armonk, New York, USA). The patients were grouped based on the initiation age of the treatment, the severity of head asymmetry, and their compliance level. The treatment effects of each group were compared using a paired sample T-test and a Wilcoxon signed rank test. The statistically significant level was set at P<0.05. The correlation between the treatment effect and the helmet wearing time was tested using a Pearson's correlation test (P<0.05). We considered a final CVA ≤5 mm to indicate a successful treatment. The changes in the successful treatment rate according to the treatment initiation age and the treatment period were analyzed using an receiver operating characteristic (ROC) curve with a 95% confidence interval (CI).
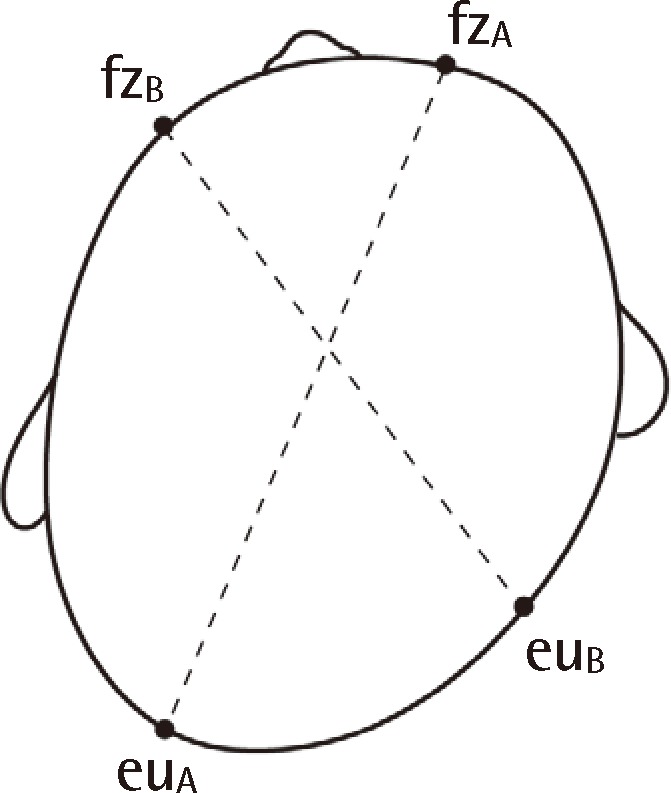
Diagonal measurement of patient's head
The frontozygomatic-to-contralateral occipital (euryon) distance was measured using spreading calipers on both sides of each patient. The distances were defined as diagonal A (fz A to eu A) and B (fz B to eu B) (A>B), after which the cranial vault asymmetry (CVA) (diagonal A to diagonal B) and cranial vault asymmetry index (CVAI) ([diagonal A to diagonal B]/[diagonal A×100]) were measured. CVA, cranial vault asymmetry; CVAI, cranial vault asymmetry index.

The effectiveness of helmet therapy according to the starting age

The effectiveness of helmet therapy according to the initial severity

The effectiveness of helmet therapy according to the helmet wearing time
RESULTS
Of the 108 patients, the mean initiation age was 9 months (range, 3 to 43 months), and the mean CVA and CVAI before the treatment were 16 mm (range, 6 to 30 mm) and 10.68% (range, 3.85% to 19.29%), respectively. The mean helmet wearing time was 17 hours a day (24 hours), and the mean treatment period was 6.6 months. The mean CVA and CVAI after the treatment were 4.7 mm (range, 0 to 10 mm) and 3% (range, 0% to 6.85%), respectively. The final CVA and CVAI significantly decreased compared with the initial CVA and CVAI (P<0.0001 and P<0.0001) (Table 1, Fig. 3). When the patients were grouped based on their treatment initiation age into group 1 (5 months or less, n=20), group 2 (6 to 8 months, n=38), group 3 (9 to 11 months, n=31), and group 4 (12 months or more, n=19), the change in their CVA and CVAI was greatest in group 1 (initial CVA to final CVA=11.6 and initial CVAI to final CVAI=8.36, P=0.0001 and P=0.0001), and least in group 4 (initial CVA to final CVA=10.7 and initial CVAI to final CVAI=6.77, P=0.0001 and P=0.0001), which meant that the treatment effect was greater in the younger patients than in the older patients (Table 1).
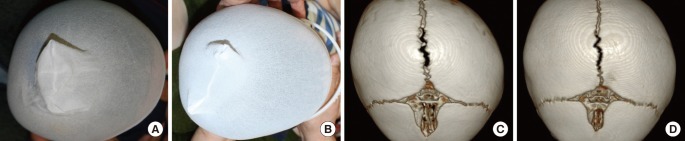
Photos and 3D CT: pre- and posttreatment
(A) The initial CVA and CVAI were 17 mm and 11.56%, respectively, which were measured using spreading calipers. (B) The CVA decreased by 12 mm (initial CVA, 17 mm; final CVA, 5 mm) and the CVAI decreased by 8.19% (initial CVAI, 11.56%; final CVAI, 3.37%). The treatment initiation age was 6.3 months and the treatment period was 7.1 months. (C) Before the helmet therapy, a three-dimensional (3D) computed tomography (CT) scan was performed to confirm that craniosynostosis was not present. In the 3D CT scan, any discrepancy in the diagonal distances was noted. (D) When the helmet therapy was over, the 3D CT scan was performed again to assess the treatment effect. The posttreatment 3D CT scan showed the decreased discrepancy of the diagonal distances. CVA, cranial vault asymmetry; CVAI, cranial vault asymmetry index.
Among the patient groups based on the initial CVA (mild [6 to 10 mm, n=15], moderate [11 to 15 mm, n=34], and severe groups [≥16 mm, n=59]), the change was greatest in the severe group (initial CVA to final CVA=14.5 and initial CVAI to final CVAI=9.8, P<0.0001 and P<0.0001) and least in the mild group (initial CVA to final CVA=5 and initial CVAI to final CVAI=3.6, P=0.0006 and P=0.0007). In addition, the treatment periods were 6.1, 5.8, and 7.1 months in the mild, moderate, and severe groups, respectively. The Pearson's correlation test of the correlation between the initial CVA and the treatment period showed that the greater the initial CVA was, the longer the treatment period was (r=0.06, P=0.040) (Table 2), and this was statistically significant.
In addition, the patients were grouped based on helmet wearing time into the poor compliance group (<15 hours, n=24), good compliance group (15 to 19 hours, n=55), and excellent compliance group (≥20 hours, n=29). In the poor and good compliance groups, the longer the helmet wearing time was, the significantly greater the initial to final CVA and initial to final CVAI were (r=0.432, P=0.0349, and r=0.266, P=0.0499); however, they were not significantly greater with longer helmet wearing in the excellent compliance group (r=-0.022, P=0.9111), according to Pearson's correlation test. These findings indicate that the treatment effect was proportional to the helmet wearing time up to 20 hours a day. However, the treatment effect was not proportional to the helmet wearing time beyond 20 hours. In addition, the treatment periods were 7.27, 6.92, and 5.29 months in the poor, good, and excellent compliance groups, respectively, which meant that the poorer the compliance level was, the longer the treatment was needed (P=0.006) (Table 3).
We considered a final CVA ≤5 mm as a successful treatment, and the rate of successful treatment was 73% (75 in total 108 patients). When the initiation age of the helmet therapy was 9.1 months, the area under the ROC curve was 0.633 which was in the 95% CI 0.535 to 0.724. This meant that the rate of successful treatment was statistically different at the point of 9.1 months (in other words, the patients who started helmet therapy younger than 9.1 months showed a higher success rate than those who started older than 9.1 months) (Fig. 4). In addition, when the treatment period of the helmet therapy was 7.83 months, the area under the ROC curve was 0.607, which was in the 95% CI 0.509 to 0.700. This means that the rate of successful treatment had a statistical difference above and below the point of 7.83 months (the patients who had worn the helmet more than 7.83 months showed a higher success rate than those who word it less than 7.83 months) (Fig. 5).
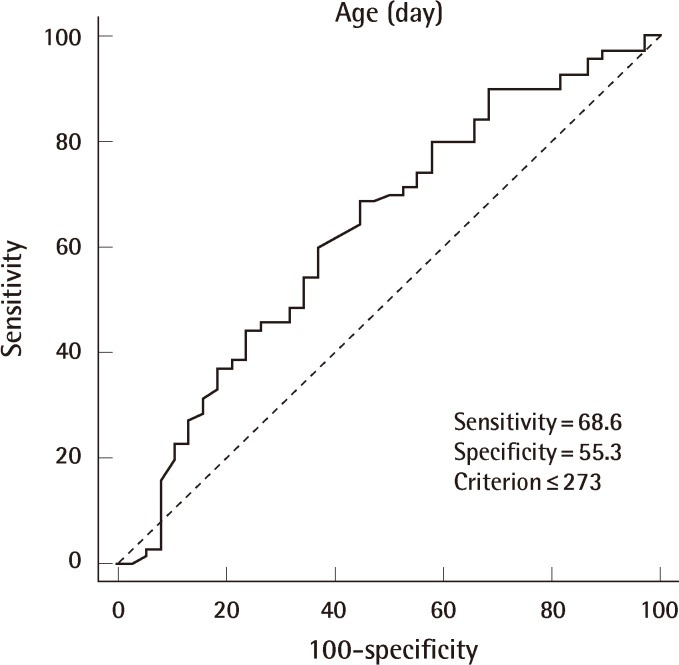
Changes of the successful treatment rate according to the age of initiation of therapy
When the initiation age of the helmet therapy was 9.1 months, the area under the receiver operating characteristic curve was 0.633, which was in the 95% confidence interval 0.535 to 0.724. This means that the rate of successful treatment was statistically different before and after the point of 9.1 months (in other words, the patients who started helmet therapy younger than 9.1 months showed a higher success rate than those who started older than 9.1 months).
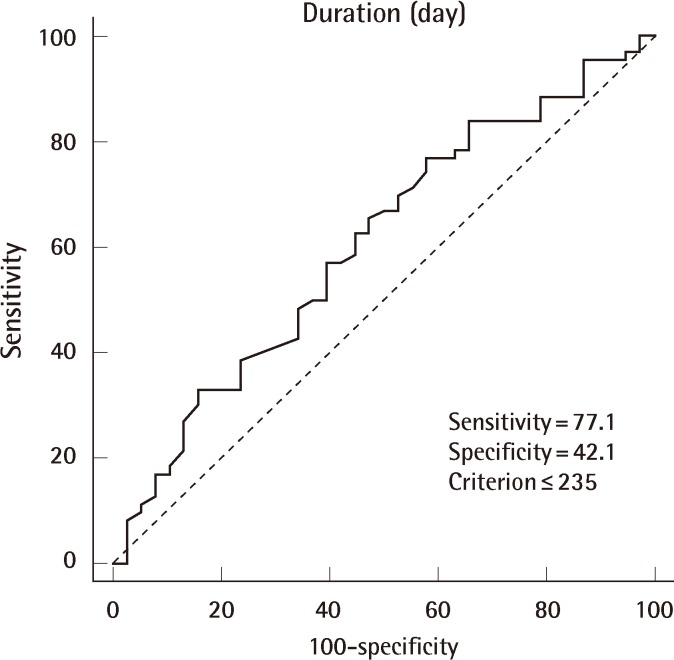
Differences in the successful treatment rate according to the duration of therapy
When the treatment period of the helmet therapy was 7.83 months, the area under the receiver operating characteristic curve was 0.607, which was in the 95% confidence interval 0.509 to 0.700. This means that the rate of successful treatment was statistically different above and below the point of 7.83 months (in other words, the patients who had worn the helmet more than 7.83 months showed a higher success rate than those who wore it less than 7.83 months).
DISCUSSION
The treatment effect of helmet therapy for nonsynostotic plagiocephaly in pediatric patients has been reported in many studies [1,6,10,13-17] since the first report by Clarren et al. [18] in 1979. It has been reported that nonsynostotic plagiocephaly would not spontaneously improve [4,5] and that complications related to helmet therapy, such as contact dermatitis, miliaria, and skin rash, were not severe [15,19,20]. However, it could be possible that helmet wearing would result in developing severe complications such as focal pressure injury. In this study, the authors reported good treatment effects of helmet therapy by comparing initial CVI and CVAI with final CVI and CVAI. However, there is no quantified standard measurement for the assessment of the outcome of helmet therapy [2]. In the previous studies, the CVA, CVAI, cranial index, orbitotragial depth asymmetry (OTDA), and cranial base asymmetry (CBA) were used for the outcome analysis [6,8,14,16,19]. Moreover, the cosmetic outcome score based on the parent's perception was also used [21]. Among these various measurements, we used CVA and CVAI because these were measured easily in the outpatient clinic using spreading calipers. Furthermore, a recent study reported that the CVAI was a suitable measurement because it was independent of the head size [19]. Although experienced physicians measured the CVA and CVAI using a spreading caliper in this study, it was possible that the measurement was changeable according to the patient's position and motion [22,23]. Thus, more advanced methods such as three-dimensional surface scanning laser therapy [13], three-dimensional photographic analysis [14], and a computer-aided design (CAD) system [2] have been introduced in recent studies, which could reduce such errors.
Although many studies have reported good results of helmet therapy, none have addressed the best initiation age of the therapy and the treatment period. In s previous study, the optimal time to start helmet therapy was months 5 to 6 of life according to the comparison of the treatment effect of two groups (one group started helmet therapy before 6 months of age and the other group started older than 6 months) [24]. However, in this study, we considered a final CVA ≤5 mm to be a successful outcome, and analysis of the change of success rate according to the initiation age and the treatment period. If the initiation age of the helmet therapy was older than 9.1 months, the rate of successful treatment decreased significantly. According to previous reports, pediatric patients are started on helmet therapy for nonsynostotic plagiocephaly older than 4 months because spontaneous correction of skull asymmetry may be possible according to brain growth up to 4 months of age [15,20]. Thus treatment initiation between 4 and 9.1 months old is considered appropriate. In the same way, the rate of successful treatment decreased significantly when the treatment period was shorter than 7.83 months.
Thus, according to the results of this study, we suggest a new strategy for helmet therapy. The strategy is that the therapy should be started between 4 and 9.1 months old, the treatment period should be more than 7.83 months, and the helmet wearing time should be more than 20 hours a day (Table 4).
Helmet therapy strategy
Of the 108 pediatric patients, 18 patients' experience coincided with this new treatment strategy. The mean initial diagonal A and B of the 18 patients were 145.9 mm and 130 mm, and the mean final diagonal A and B were 155.1 mm and 150.4 mm. Based on these results, diagrammatic representation of the treatment effect of the treatment strategy is presented (Fig. 6). This helmet therapy strategy may be a practical guideline for the treatment for physicians and patients' parents.
The treatment effect of the helmet therapy strategy
Only 18 of the 108 patients' experience coincided with the new treatment strategy. The mean initial diagonal (A) and (B) of these 18 patients were 145.9 mm and 130 mm, respectively, and the mean final diagonal (A) and (B) were 155.1 mm and 150.4 mm, respectively. The diagrammatic representation of the treatment effects is shown in the figure on the right.
Notes
This article was presented at the 69th Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 11-13 2011 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.