Management of Foreign Object Migration and Surgical Removal with C-Arm Fluoroscopy
Article information
The entry of a foreign object into a human body is a very common event. Workers who use sharp tools such as needles often meet with accidents. In Korea, acupuncture needles are very common sharp materials that can cause the entry of a remnant foreign object into a human body. The management of sharp foreign objects embedded in the head or neck area by early surgical removal is recommended [1]. We had a case of accidental needle breakage that caused a remnant foreign object to enter the buccal area. The purpose of this case report is to share the findings of this case with other practitioners.
A 52-year-old female patient with a foreign object embedded in her left cheek visited our plastic surgery clinic with complaints of pain and swelling. Although the object was not palpable on the skin, she felt tenderness. She used to perform acupuncture using blood lancet needles on her body by herself without a license. One of these needles broke when she was performing acupuncture on her cheek. This needle fragment advanced further away to the soft tissue.
Simple X-ray identified the needle embedded in her left cheek (Fig. 1). To precisely evaluate the location and the depth of this embedded object, ultrasonography was performed. From the ultrasound image, we found that the needle had traveled 1 cm from the opening to a soft tissue area (Fig. 2).

Preoperative simple X-ray (white arrow points to the embedded needle).
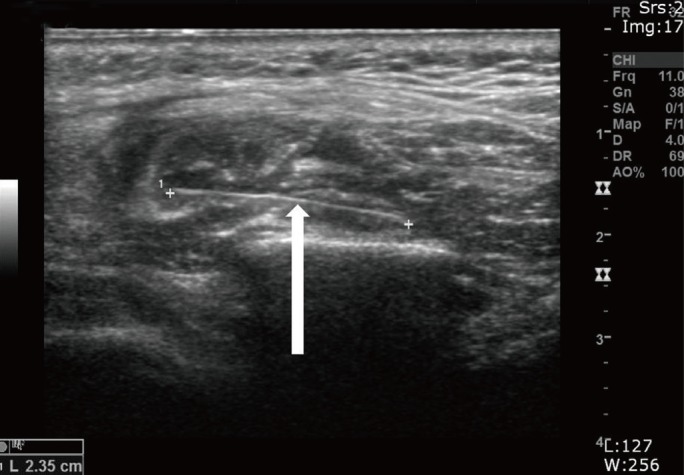
Preoperative ultrasound image (white arrow points to the embedded needle).
We scheduled a removal operation for the following day. The next day, the patient was laid on an operating table under local anesthesia. First, we made a 1-cm-long incision on the skin and tracked the needle from the opening by using C-arm fluoroscopy. The needle was successfully removed using a straight mosquito clamp under C-arm fluoroscopy (Fig. 3). There was no complication such as hematoma or numbness after the removal operation.
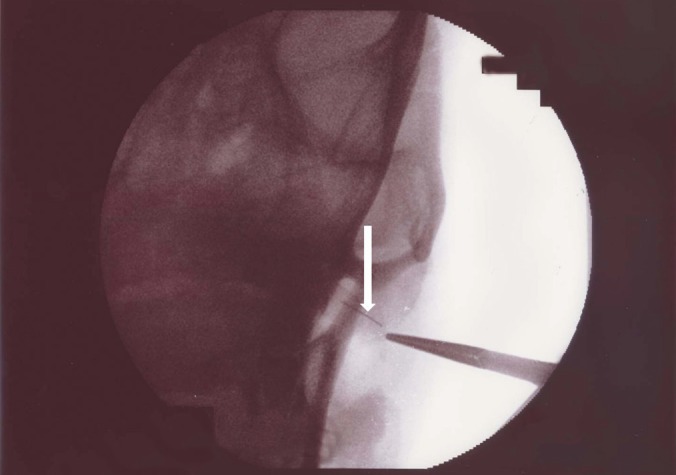
Intraoperative C-arm fluoroscopy image (white arrow points to the embedded needle).
Medical doctors, particularly surgeons, frequently experience patients with remnant foreign bodies. Acupuncture procedures are commonly performed by unlicensed practitioners in Korea. Using computed tomography (CT) and/or ultrasonography, many Korean medical practitioners have found remnant foreign objects such as Hari acupuncture needles embedded in patients. However, very often, these patients do not have any symptoms or sequelae of acupuncture needle migration [2].
A remnant foreign object, particularly a sharp object such as a needle or a fish bone, has many potential risks. Such an object may cause injury to adjacent structures or migrate to another location from which it may be difficult to remove [3]. Some foreign objects can remain embedded in the tissue or another structure without symptoms or complications for many years [4].
Surgeons should refrain from a rushed exploration without preoperative evaluation to determine the exact location of the foreign body or the proximity of corresponding critical structures because there is a high probability of causing injury to an adjacent structure [1]. We can use simple X-rays to locate the foreign body first. However, X-rays have very low sensitivity in detecting foreign bodies [3]. Three-dimensional CT is an excellent tool for identifying the location of an embedded foreign body. However, CT is associated with a greater radiation dosage [5]. Another imaging option is ultrasound. It can localize an embedded foreign body preoperatively and intraoperatively [3]. The location of a foreign body can also be intraoperatively visualized by using C-arm fluoroscopy.
We first evaluated the location of the foreign body preoperatively by simple X-ray and ultrasound. We found that the foreign body was 1 cm away from the opening. The next day, we performed the removal operation using C-arm fluoroscopy. However, the foreign body had migrated by another 1 cm away from the opening, even though we warned the patient not to speak or chew too much to prevent needle migration, which might be caused by facial muscle contraction. Therefore, when we performed the removal operation, the embedded needle was located 2 cm away from the opening (Fig. 4).
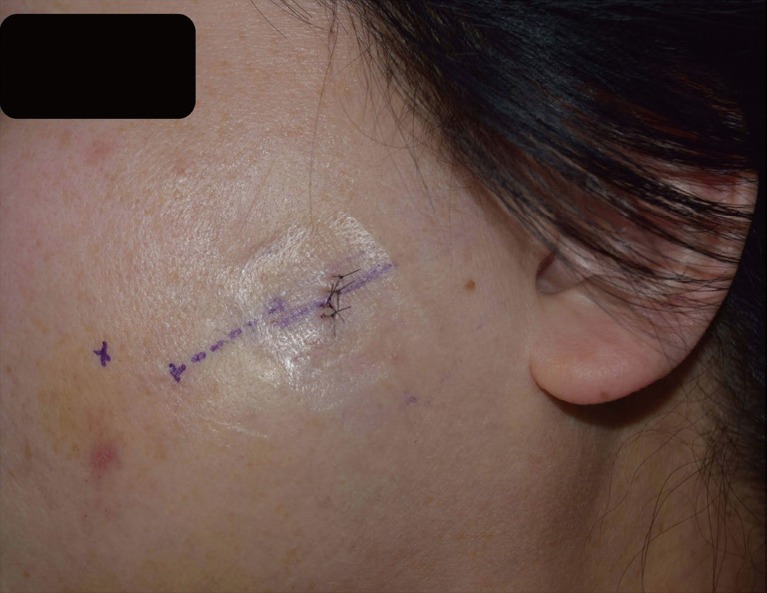
Postoperative photograph ("X" mark, original skin opening; dotted line, preoperatively evaluated location of the needle; solid line, migrated location of the needle).
In this case, the embedded foreign body had migrated. Acupuncture needles, fish bones, and broken dental needles are very hazardous foreign bodies that can migrate to other locations. Such migration can cause injury to critical structures or cause the foreign body to move to a deep layer where it may be difficult to remove. Almost all articles and case reports published thus far on this topic have reported the necessity of early surgical removal if the patient has exhibited any symptoms, irrespective of the size of the foreign object and its location with respect to a critical structure. Thus, early surgical removal of a sharp foreign object is important to minimize the risks that might be caused by the foreign body.
There are many unlicensed individuals who perform acupuncture using unsafe materials, which can potentially lead to infections and can cause confusion with respect to the identification of the actual material of the embedded foreign object (Fig. 5). The embedded foreign body is likely to migrate, particularly in the facial area. Moreover, such migration may cause a critical injury. We are deeply concerned about the reality of the practice of acupuncture with inappropriate materials in certain cases. In light of the case presented here, we wish to direct the clinician's attention to the risk of migration of an unsafe foreign object used in acupuncture and the need for an urgent removal operation, particularly when the object is embedded in the facial area.
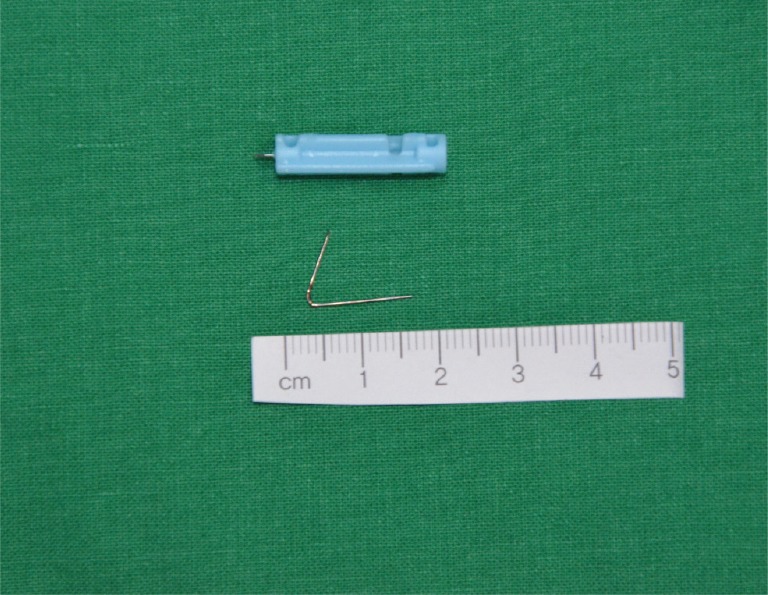
Removed foreign body (blood lancet needle).
Notes
No potential conflict of interest relevant to this article was reported.