Solitary Gluteus Maximus Muscle Metastasis in a Breast Cancer Patient
Article information
Tumor metastasis into skeletal muscle is uncommon, and is rarely noticeable clinically. Lung cancer and gastrointestinal tumors are the most frequent primary malignancies that metastasize to the skeletal musculature, but some reports have described muscle metastases from breast cancer [1]. The authors present a case of gluteal muscle metastasis in a patient with a known primary breast cancer.
A 53-year-old woman presented with a mass on her right buttock with pain that was aggravated by walking. She had previously undergone modified radical mastectomy due to left breast cancer. A histopathological examination at the time had shown invasive ductal carcinoma without axillary lymph node metastasis. She had received five cycles of adjunctive chemoradiotherapy with cyclophosphamide, methotrexate, and 5-fluorouracil, followed by tamoxifen. Seven years after surgery, a slowly growing mass developed on her right buttock with mild throbbing pain. On physical examination, tenderness was observed, but no palpable mass was found in the right buttock. A computed tomography (CT) examination of the pelvis found a poorly defined, mildly enhanced intramuscular mass measuring 3 cm in the patient's right gluteal maximus muscle (Fig. 1), and a subsequent needle biopsy of the lesion confirmed a metastatic, poorly differentiated invasive ductal carcinoma. In order to address suspicion of systemic metastasis, the patient underwent CT scans of the breast, positron emission tomography-CT, and bone scans. No other metastatic sites were found (Fig. 2). A wide excision and local flap coverage were performed to remove the metastatic mass along with tissue from the gluteus muscle (Fig. 3). Histological findings showed metastatic invasive ductal carcinoma (Fig. 4). She received adjunctive chemotherapy with capecitabine and no local recurrence was observed 12 months after surgery.
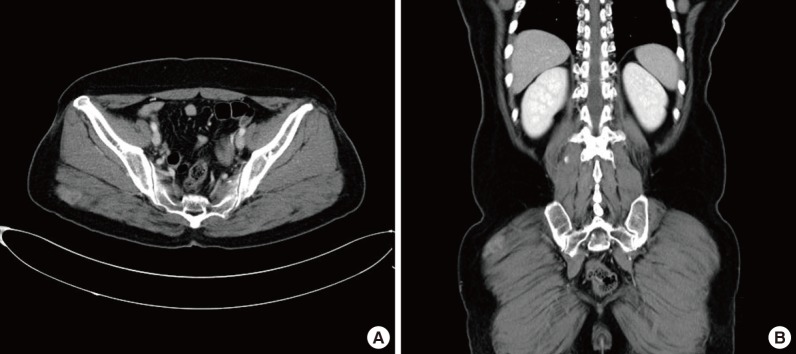
(A, B) Preoperative computed tomography views. An enhancing mass is visible in the right gluteus maximus muscle, suggesting an intramuscular metastasis.
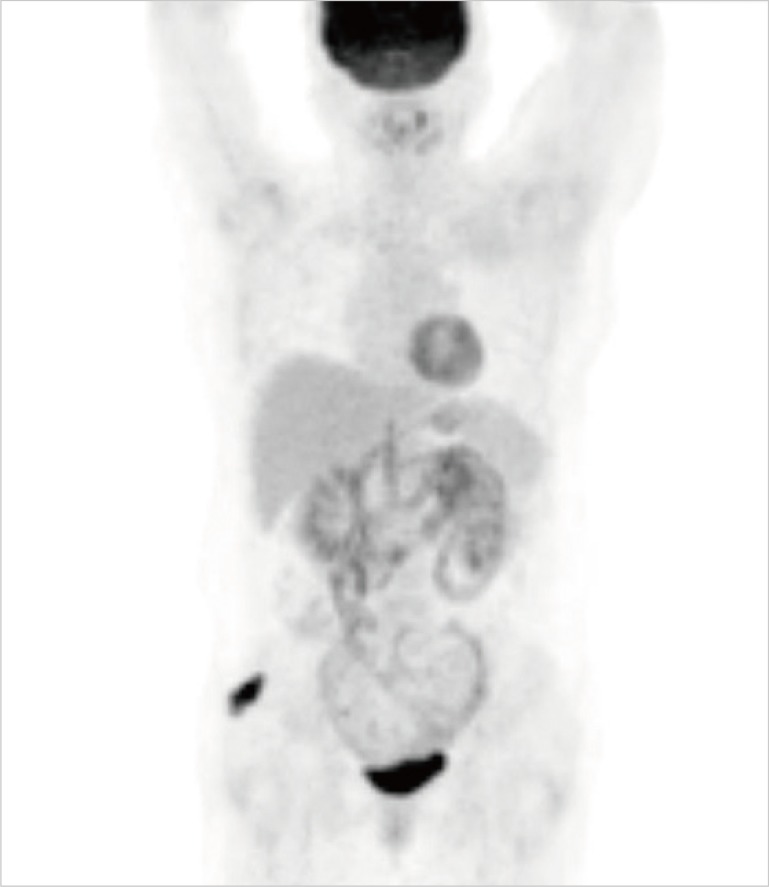
Preoperative positron emission tomography-computed tomography (PET-CT) view. PET-CT revealed a significant hypermetabolic lesion in the right gluteal muscle. No other suspected metastatic sites were found.
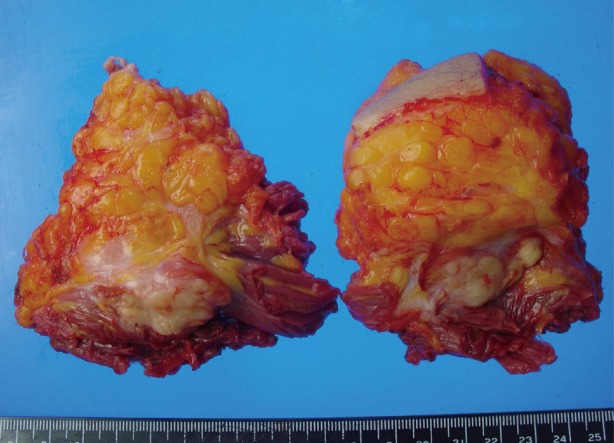
Gross photo of the resected intramuscular mass.
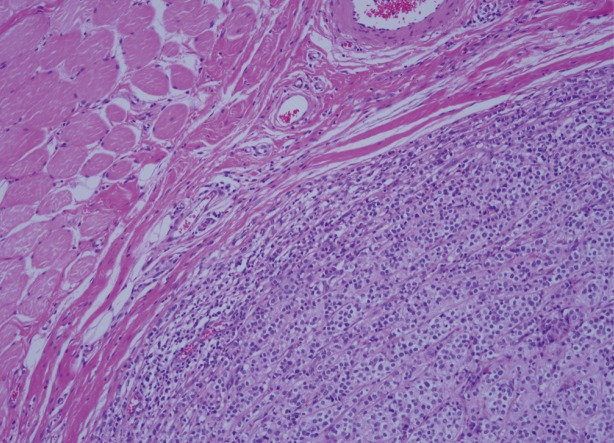
Histological findings of the surgical specimen. Metastatic invasive ductal carcinoma had infiltrated into the surrounding muscle (H&E, ×100).
Skeletal muscle metastasis of a primary malignancy is relatively rare and can be misdiagnosed as a primary soft tissue sarcoma; however, distinguishing between the two diagnostic possibilities is critical, because the treatment and prognosis may differ markedly [1].
Metastases of breast cancer may appear in any organ, and although different relapse sites may be observed depending on the subtype of breast cancer, the most frequent metastasis sites are bone, the liver, the lungs, and the brain [2]. Skeletal muscle metastasis of breast cancer is very rare. The following sites have been reported for skeletal muscle metastasis: the abdominal wall muscle, the iliopsoas muscle, the gluteus medius muscle, the triceps muscle, the scalene muscle, the extraocular muscle, the cervical muscle, and the paraspinal muscle [3]. The gluteus maximus muscle has not been reported as a site of skeletal muscle metastasis. It has not been clearly established why tumor metastasis is so rare in skeletal muscle, despite its abundant vascular supply. However, one possible reason is that muscle contractions, in combination with variable but abundant vascular flow, may mechanically prevent tumor cells from stopping and proliferating. It also appears that the settlement and growth of tumors are not favored in muscle tissue due to its pH value and a chemical environment driving the degradation of lactic acid, an angiogenesis-promoting agent [3].
The most common symptom is pain at the metastatic site, although skeletal muscle metastasis is manifested as the formation of a tumor mass and muscle weakness [3]. If a patient presents with mild pain without clear evidence of a mass upon physical examination, as occurred with the patient in this case, the metastatic tumor may be easily missed. Therefore, careful diagnosis is required.
The prognosis and appropriate treatment of skeletal muscle metastasis are uncertain. A previous report recommended that skeletal muscle metastases be treated palliatively if they occur together with systemic metastasis, but an isolated metastatic neoplasm can be resected operatively with or without radiotherapy [34].
Although some authors have proposed performing contralateral prophylactic mastectomy, randomized controlled trials to assess the overall survival benefit of this procedure in breast cancer patients have never been carried out, and its efficacy is therefore unclear [5].
This report presented a rare case of a breast cancer metastasis into the gluteal muscle that was completely resected operatively after confirming the diagnosis with a preoperative needle biopsy. In patients with an intramuscular mass, it is necessary to proceed with a suspicion of metastatic cancer, even though metastasis to muscle tissue is rare.
Notes
No potential conflict of interest relevant to this article was reported.