Traumatic Carotid-Cavernous Sinus Fistula in a Patient with Facial Bone Fractures
Article information
Carotid-cavernous sinus fistulas (CCFs) are abnormal connections between the cavernous sinus and the carotid arterial system (the internal carotid artery, external carotid artery, or both). CCFs may be classified as spontaneous or acquired and as direct (high blood flow) or dural (low blood flow) [1]. Direct CCFs represent 70% to 90% of all CCFs, and mostly result from head trauma, especially basal skull fractures [2]. Patients with CCFs may present with signs and symptoms such as conjunctival chemosis, decreased vision, proptosis, diplopia, orbital pain, audible bruits, headache, and blindness [23]. In this report, we present the case of a 49-year-old man with a CCF and ophthalmic symptoms, resulting from a left zygomaticomaxillary complex fracture.
The patient presented with left facial swelling, numbness, orbital pain, and severe headache caused by an unknown injury. A physical examination revealed limited extrinsic ocular motility (vertical movement), diplopia, exophthalmia, dilated conjunctival vessels, and conjunctival chemosis of the left eye (Fig. 1). Slightly decreased vision in his left eye was noted. An elevated intraocular pressure (27 mm Hg) was also observed in the left eye. Brain computed tomography (CT) was immediately performed, and epidural hemorrhage and pneumocephalus were detected. Facial bone CT revealed a zygomaticomaxillary complex fracture and a basal skull fracture with left sphenoid sinus wall fractures (Fig. 2). After conservative treatment for the intracranial hemorrhage in the intensive care unit, the patient's condition stabilized without neurologic complications. Open reduction and internal fixation of the facial bone fractures was performed 18 days after the injury. A left periorbital hematoma was meticulously removed. The patient's general symptoms gradually improved after surgery. However, chemosis and headache persisted. Enhanced CT of the brain and angiography of both the external and internal carotid arteries were performed to evaluate the possibility of other intracranial lesions. Enhanced CT showed abnormally increased enhancement of the superior ophthalmic vein (Fig. 3). Angiography of the left internal carotid artery showed abnormal anterior drainage into the left superior and inferior ophthalmic veins (Fig. 4). Transarterial endovascular embolization therapy through femoral artery access was performed to occlude the fistula. Three months after the embolization, although left inferior hemianopsia persisted as a sequela of the CCF, the subjective and objective ophthalmic symptoms had resolved (Fig. 5).
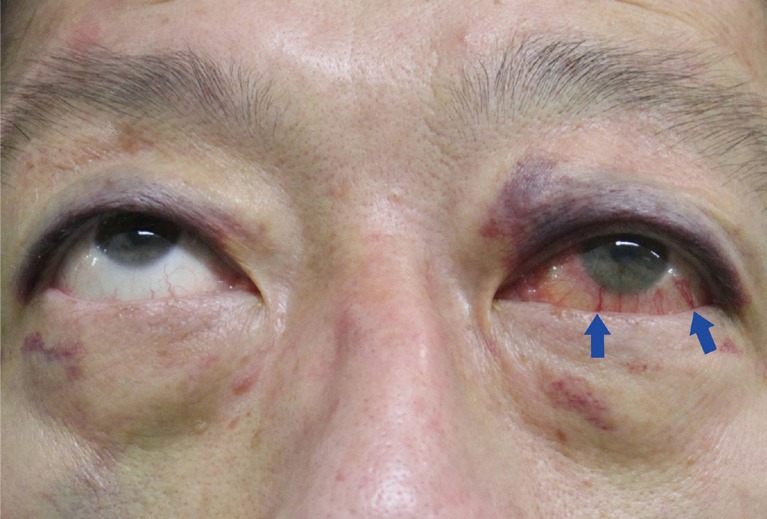
Preoperative characteristics. A 49-year-old man with limited upward gaze, proptosis, and conjunctival chemosis of the left eye. Episcleral venous engorgement of the left conjunctiva (blue arrows) can be seen.
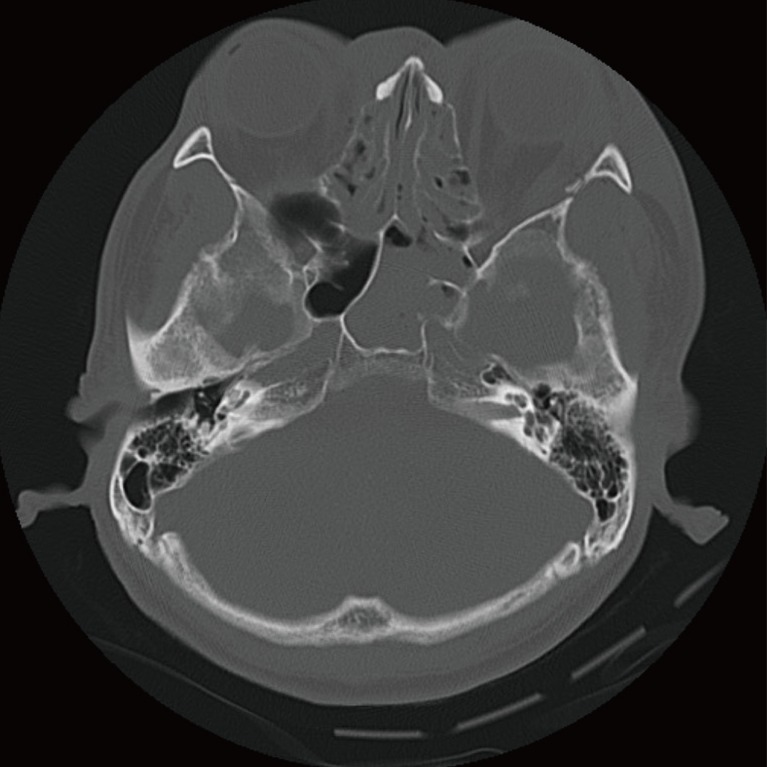
Computed tomography of the facial bone showing a sphenoid sinus fracture with air-fluid level.
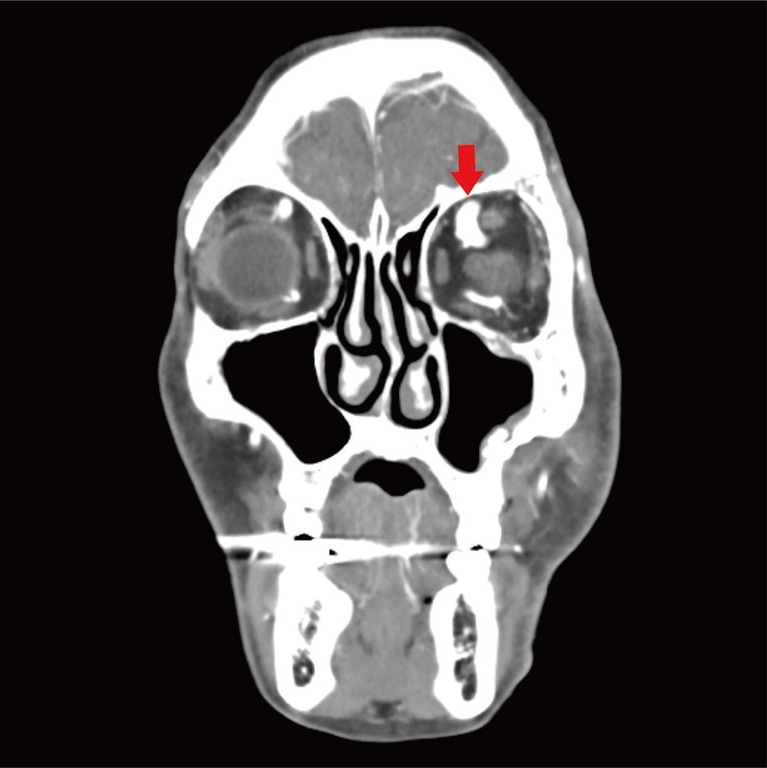
Enhanced computed tomography of the facial bone showing an enlarged left superior ophthalmic vein (red arrow).
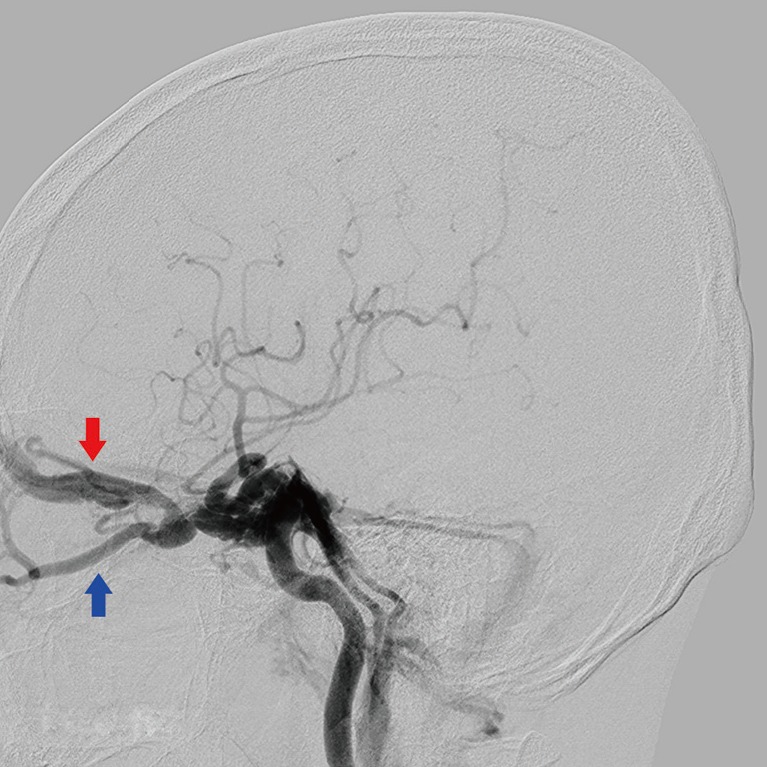
Angiography of the left internal carotid artery showing abnormal anterior drainage into the left superior (red arrow) and inferior (blue arrow) ophthalmic veins.

The left eye of the patient three months after the operation, after full recovery.
CCF is a rare complication of craniofacial fractures, occurring in only 0.17% to 0.27% of cases [3]. Since untreated fistulas can lead to progressive ocular symptoms and eventually to total loss of visual acuity and ischemic optic neuropathy [23], the early diagnosis of CCFs is important. However, the diagnosis is often difficult due to ambiguous ocular symptoms and accompanying severe brain injuries [3]. These fistulas have even been observed in patients with facial bone fractures, especially those involving the sphenoid sinus and orbital wall [34]. Therefore, CCFs should be suspected in patients with craniofacial injuries and complex ocular symptoms such as sustained chemosis, exophthalmos, dilation of the episcleral veins, decrease in visual acuity, or elevated intraocular pressure [3]. Although the enlargement of the cavernous sinus and extraocular muscle or dilation of the ophthalmic vein is suggestive of CCFs, the gold standard for the diagnosis of CCFs is cerebral angiography [5]. The goal of treatment is to occlude the fistula site by a range of possible methods. Conservative therapy, such as external manual compression of the ipsilateral cervical carotid artery and radiosurgical intervention, may be effective for CCFs with low blood flow [5]. However, endovascular embolization through transarterial or transvenous access using metallic coils, with or without liquid embolic agents, is the first line of treatment for CCFs with high blood flow [5]. Open surgical intervention should be performed in cases where endovascular treatment is not possible or is unsuccessful [5]. After successful occlusion of the fistula, symptoms such as conjunctival chemosis and proptosis generally improve within hours to days [135]. Cranial nerve palsies often resolve within several weeks [5]. The recovery of vision largely depends on the severity of the injury before intervention [5].
This case highlights the importance of the diagnosis and treatment of CCFs in patients with a facial bone fracture accompanying a basal skull fracture. Since serious sequelae, such as irreversible visual loss, can result from CCFs, the early detection of alarming signs and symptoms in patients with facial bone and basal skull fractures could prevent permanent disability and improve treatment outcomes. Therefore, we recommend that ocular examinations should be performed in patients with craniofacial injuries and symptoms suggestive of CCFs. Moreover, radiologic modalities for the diagnosis and treatment of CCFs, such as CT scans and cerebral angiography, should be considered.
Notes
No potential conflict of interest relevant to this article was reported.
This article was presented as a poster at the Fifth Research and Reconstructive Forum of the Korean Society of Plastic and Reconstructive Surgeons on May 14-15, 2015, in Pyeongchang, Korea.