Giant Fibroadenoma in the Axilla: A Common Entity of Uncommon Size in a Rare Location
Article information
A 20-year-old patient presented at our department with a slow-growing mass spanning from her right axilla to the medial upper arm. She had first noted the asymptomatic mass 10 months previously. Physical examination revealed a firm but relatively mobile mass measuring 8 cm×2 cm in the right upper medial arm. The mass was painless and nontender, with no fluctuation. No neurological signs and no infection signs with respect to the right arm were observed (Fig. 1). Computed tomography showed a lobulated mass measuring 8.5 cm×4.0 cm×2.1 cm with intermediate density in the subcutaneous layer of the right axilla and the upper medial arm (Fig. 2). Under the impression of a soft-tissue tumor of nerve origin, an excisional biopsy was performed through an axillary incision. A well-encapsulated, lobulated, pink, rubbery mass was found in the deep subcutaneous fat layer and was excised from the surrounding tissue (Fig. 3). Histopathologically, a biphasic pattern of epithelial and stromal proliferation was noted. The ductal epithelium was composed of an inner cuboidal/columnar epithelium and an outer myoepithelial layer. The fibrous stromal tissue showed an intracanalicular growth pattern, corresponding to the diagnosis of fibroadenoma (Fig. 3). The patient underwent sonography evaluation for any lesions in both breasts with negative findings.
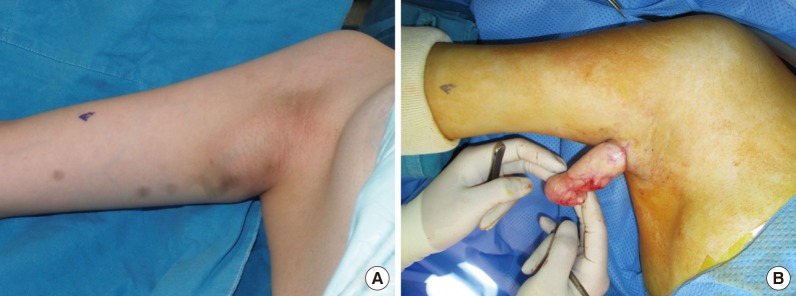
Preoperative and intraoperative findings. (A) The bulging, palpable mass spanning from the right axilla to the upper portion of the arm is seen preoperatively. (B) A well-encapsulated, pink, rubbery, and lobulated mass was found.

Computed tomography findings of a lobulated mass measuring 8.5 cm×4.0 cm×2.1 cm with intermediate density in the subcutaneous layer of the right upper medial arm and the axilla.
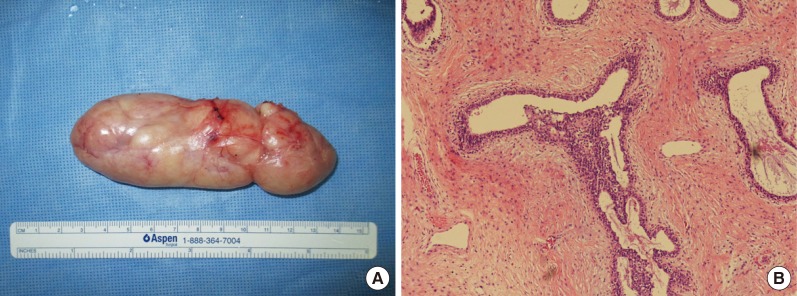
(A) The excised specimen measuring 11.5 cm×5 cm. (B) Histological findings of both epithelial hyperplasia and stromal hypercellularity (H&E, ×100).
Fibroadenoma is a benign, fibroepithelial tumor of the breast. While a vast majority of these tumors have been found in females, rare occurrences have been reported in males [1]. Due to their benign nature, some have thought that these lesions are not neoplasms but hyperplastic lesions. However, recent studies observing the transformation of breast fibroadenoma to malignancies have reported differently. Pacchiarotti et al. [2] reported the transformation of fibroadenoma into high-grade malignant tumors after ovarian stimulation in in vitro fertilization patients.
Specific variants of fibroadenoma include giant fibroadenoma, juvenile fibroadenoma, multiple fibroadenomas, and fibroadenoma of pregnancy and lactation. Giant fibroadenomas have a diameter of more than 5 cm and/or weigh more than 500 g, as in this case. Multiple fibroadenomas are associated with a related family history or several cancer syndromes such as the Maffucci syndrome, Cowden syndrome, and Carney complex [3]. Juvenile fibroadenoma usually presents as a breast mass in patients between the age of 10 and 18 years. Jung et al. [4] reported a case found in a 13-month-old child, but such incidence is extremely rare. The incidence of breast lesions in the general adolescent population is low (2.2%), and a majority of these lesions are fibroadenomas.
Definitive diagnosis is done through histopathological examination. Ultrasonography may help distinguish between solid and cystic lesions of the breast, and fibroadenomas typically have a longer width than height, surrounded by an echogenic capsule. Fine-needle aspiration is not reliable in distinguishing a fibroadenoma from a phyllodes tumor. Core-needle biopsy has strong negative (93%) and positive (83%) predictive power, but only by histopathological examination of the entire specimen can a definite diagnosis be made.
The pathophysiology of this entity has not been fully established. Hormonal influences have been suggested to be a factor, due to the increase in prevalence during puberty or pregnancy, or during the intake of oral contraceptives. Suggested hypotheses are an imbalance of estrogen levels or hypersensitivity of breast tissue to estrogen, resulting in mammary gland hyperplasia [5]. Thus, a vast majority of fibroadenomas are found in the breast. Although there have been rare reports of lesions found in the axilla, this is the first report of a fibroadenoma of this dimension solitarily occurring in the axilla [5]. In this report, we have included the relevant clinical, gross, and micrographic pathological images.
Notes
No potential conflict of interest relevant to this article was reported.