Leiomyoma on Nasal Dorsum
Article information
Leiomyomas are benign tumor of smooth muscle origin, most commonly found in the uterus and gastrointestinal tract [1]. Less than 1% happen in some head and neck structure [2]. Especially, they are rare in nose because of paucity of smooth muscle. Almost those cases are usually confined to the subcutaneous tissue and skin, rarely occurring in the deep tissue. We report a 10-year-old female with leiomyoma of the nasal dorsum arising from the deep tissue.
A 10-year-old female was referred to our hospital with a slowly increase in the size of mass for the last 4 years. She has no history of trauma in the years just before the tumor was recognized. Physical examination showed a oval shaped 1.5×1 cm mass on the right nasal side wall, which was non movable and tenderness to palpation (Fig. 1). Contrast enhanced computed tomography revealed an oval-shaped nodule that was located in the right nasal dorsum subcutaneous fat layer, most suspected dermoid cyst. It was very close to the nasal bone, but there was no bony erosion and destruction (Fig. 2).

Preoperative photographic finding shows a 1.5×1 cm sized oval shaped mass on the right nasal lateral wall in a 10-year-old girl.
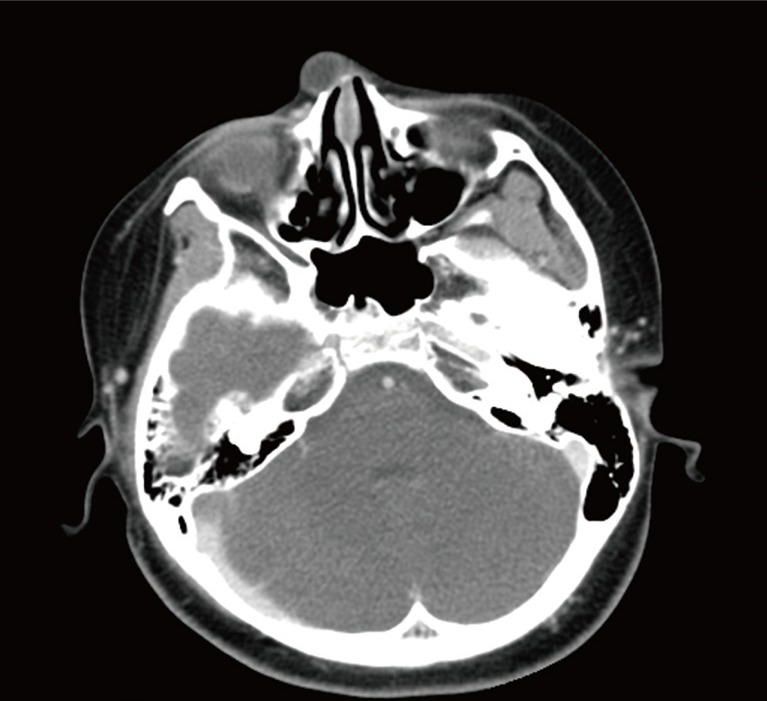
Axial enhanced computed tomography scan shows an oval-shaped nodule that was located in the right nasal dorsum subcutaneous fat layer, close to the nasal bone.
The mass was excised using a direct incision under general anesthesia. In operation, the mass are adhered to the skin, fascia and small vessels. The mass including attached skin was separated from the underlying nasalis muscle. We biopsied the lesion and the pathology report classified it as a leiomyoma with degeneration change in central area, confirmed based on the immunohistochemistry showing desmin negativity and smooth muscle actin positivity (Fig. 3). After the resection of the lesion, the patient underwent an observation of 3 months' follow-up, and no recurrence was detected (Fig. 4).

(A) Microscopic findings shows bundles of smooth muscle cells with collagen fibers with degeneration change in central area (H&E, ×40). (B) Immunohistochemical finding shows positivity for smooth muscle actin (×200).

Postoperative 3 months photographic finding reveals removal of the nasal lateral wall mass, no recurrence was detected.
Soft tissue leiomyomas can be subdivided into three distinct groups. The most common form, the cutaneous leiomyoma, arises from the erector pili muscles of the skin and the deep dermis of the scrotum, labia major, and nipple [3]. The second group of soft tissue leiomyomas, the angioleiomyomas (also known as angiomyomas or vascular leiomyomas), are differentiated by their subcutaneous location and histology, which is characterized by a conglomeration of thick-walled vessels associated with smooth muscle tissue. These are solitary lesions and most commonly present in the adult, with two thirds occurring in the fourth through sixth decades. These lesions are typically small (<2 cm) and located in the extremities [3]. The third group, leiomyomas of the deep soft tissues, may be located in the deep soft tissues of the extremities or the retroperitoneum. The retroperitoneal variety is more commonly found in females, possibly reflecting an origin from hormonally sensitive smooth muscle. Deeper lesions are usually larger, probably because of a delay in detection, and frequently present carried histological alterations, more likely to be confused with leiomyosarcoma [3].
Prior to our report, some cases were reported, but almost nasal cavity and paranasal sinus, in the second group. In our case, younger patient has an isolated, nodular soft tissue mass in the external nose that was large enough to approaching the nasal bone imaged with CT. It was a nonvascular leiomyoma originating from deep tissue, with degeneration change.
Among the soft tissue tumors in the head and neck area, 96% area known to be benign, and leiomyomas comprise only 1.3% of them [4]. Although there are no malignant degeneration report, the presence of benign areas of leiomyoma within leiomyosarcoma specimens raises such a possibility [1]. Recently, immunohistochemistries with mitosis-specific reagent phosphohistone-H3 and Ki-67 were even reported because of the differentiated surgical plan [5]. Therefore, leiomyoma must be differentiated from neurofibroma, angiofibroma, schwannoma, myofibroma, leiomyosarcoma, and surgical excision with postoperative histopathologic analysis should be considered.
Notes
This work was supported by the Soonchunhyang University Research Fund.
No potential conflict of interest relevant to this article was reported.