The Importance of Multidisciplinary Management during Prenatal Care for Cleft Lip and Palate
Article information
Abstract
Background
The prenatal ultrasound detection of cleft lip with or without cleft palate (CL/P) and its continuous management in the prenatal, perinatal, and postnatal periods using a multidisciplinary team approach can be beneficial for parents and their infants. In this report, we share our experiences with the prenatal detection of CL/P and the multidisciplinary management of this malformation in our institution's Congenital Disease Center.
Methods
The multidisciplinary team of the Congenital Disease Center for mothers of children with CL/P is composed of obstetricians, plastic and reconstructive surgeons, pediatricians, and psychiatrists. A total of 11 fetuses were diagnosed with CL/P from March 2009 to December 2013, and their mothers were referred to the Congenital Disease Center of our hospital. When CL/P is suspected in the prenatal ultrasound screening examination, the pregnant woman is referred to our center for further evaluation.
Results
The abortion rate was 28% (3/11). The concordance rate of the sonographic and final diagnoses was 100%. Ten women (91%) reported that they were satisfied with the multidisciplinary management in our center.
Conclusions
Although a child with a birth defect is unlikely to be received well, the women whose fetuses were diagnosed with CL/P on prenatal ultrasound screening and who underwent multidisciplinary team management were more likely to decide to continue their pregnancy.
INTRODUCTION
Cleft lip with or without cleft palate (CL/P) is one of the most common congenital facial malformations and has an incidence of one to two cases per 1,000 live births [1234]. It is especially common in Northeast and Central Asia, and two babies per 1,000 live births (males, 1.95; females, 2.20) are affected by this malformation in South Korea [5].
Since Christ and Meininger [6] first detected CL/P using prenatal ultrasound in 1981, prenatal ultrasonographic examinations have been performed routinely in Korea at the gestational age of 16 to 24 weeks. The accuracy of these examinations has increased as ultrasonographic technology and screening techniques have improved [78]. According to published reports, the sensitivity of this approach is 71%–95% [23789].
Strong negative attitudes exist throughout the world towards children with birth defects, especially towards those with physical deformities. In South Korea, the rate of artificial termination of pregnancy for reasons including maternal morbidity, sexual assault, incest, or fetal abnormalities was reported to be 19.6% in 2005, which was higher than in the corresponding rate in other developed countries [10]. In Korea, abortion is permitted only in cases of maternal morbidity, sexual assault, incest, or fetal abnormalities. Therefore, the 19.6% rate of artificial termination of pregnancy only reflected legal cases of abortion, and a much higher actual rate would be expected if all cases of abortion were taken into account.
Nusbaum et al. [11] found that the prenatal detection of CL/P did not increase the rate of pregnancy termination. Such detection could be of tremendous assistance in preparing the parents for the physical and psychological aspects of care for a child with CL/P in a timely manner.
We hypothesized that women would be likely to terminate pregnancies diagnosed with fetal CL/P. In this study, we evaluated the accuracy of the prenatal ultrasound screening for CL/P, investigated the types of assistance and care that can be provided by a multidisciplinary team composed of plastic and reconstructive surgeons, obstetricians, pediatricians, and psychiatrists in our Congenital Disease Center, and assessed the effects of this care on parental decision-making.
METHODS
Our institutional review board approved the study. A total of 11 pregnant women were included in this retrospective chart review study. The fetuses were diagnosed with CL/P and the mothers were referred to the Congenital Disease Center in our hospital from March 2009 to December 2013.
Multidisciplinary approach
The multidisciplinary team of the Congenital Disease Center for mothers of children with CL/P is composed of obstetricians, plastic and reconstructive surgeons, pediatricians, and psychiatrists (Fig. 1). When CL/P is suspected during the prenatal ultrasound screening examination, the pregnant woman is referred to our center for further evaluation.
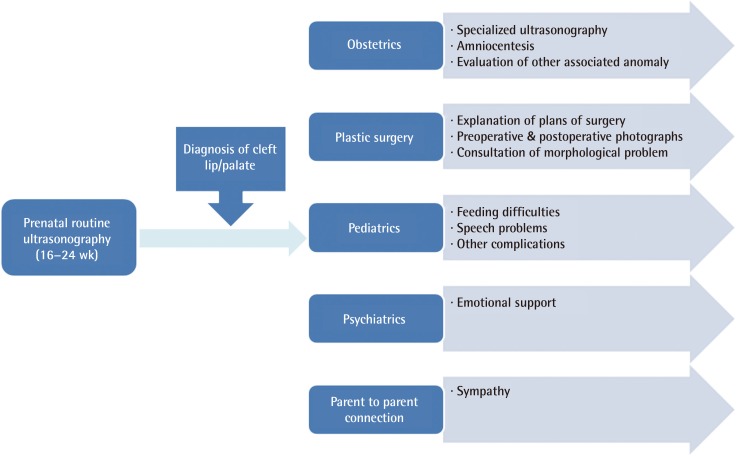
Flow diagram of the multidisciplinary management
Flow diagram of the multidisciplinary management of cleft lip with or without palate diagnosed during routine prenatal ultrasonographic examinations at the gestational age of 16–24 weeks in our institution.
Amniocentesis is performed to detect possible associated anomalies and chromosomal abnormalities in the Department of Obstetrics. The Department of Plastic and Reconstructive Surgery can provide information about surgical plans and procedures, including photographs of other children with CL/P. In the Department of Pediatrics, the parents can prepare for anticipated feeding problems and hearing difficulties. The psychiatrists provide psychological support for dealing with the feelings of guilt and frustration experienced by the parents. The parents may also be enrolled in the parents-to-parents connection program for mutual support.
Prenatal ultrasonography accuracy
CL/P cases were classified into CL (cleft lip only) and CL+P (cleft lip accompanied with cleft palate) and categorized as unilateral or bilateral during the prenatal ultrasound screening. The diagnosis was confirmed after birth by the plastic surgeons and pediatricians via physical examination, and the rate of concordance between the ultrasound screening and the ultimate diagnosis was investigated.
Satisfaction with the multidisciplinary management after the prenatal diagnosis of CL/P
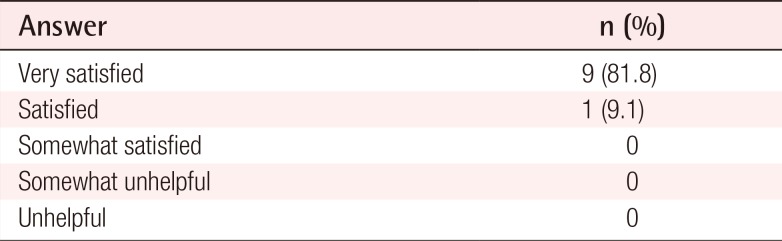
The satisfaction of the parents with the multidisciplinary care received in the Congenital Disease Center was rated using the following five-item scale: very satisfied, satisfied, somewhat satisfied, somewhat unhelpful, and unhelpful.
RESULTS
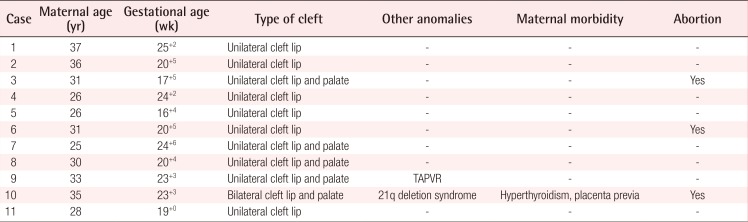
The demographic data of the patients are shown in Table 1. The average age of the mothers was 30.7 years. The diagnosis of CL/P was usually made at gestational week 21+3. With the exception of one woman who had hyperthyroidism and placenta previa, the mothers had no health problems that could have critically affected their babies. There were six cases of unilateral CL, four of unilateral CL+P, one of bilateral CL+P, and no cases of bilateral CL. One fetus was diagnosed with 21q deletion syndrome and another had associated total anomalous pulmonary venous return. Eight babies were born otherwise healthy, and three out of the 11 mothers decided to terminate their pregnancies. Thus, the abortion rate was 28% (3/11; cases 3, 5, and 10). Case 10 was aborted due to severe bilateral cleft lip and palate with chromosomal anomalies and the maternal morbidity of placenta previa. In cases 3 and 5, the parents decided to abort because of CL/P with no other comorbidity.
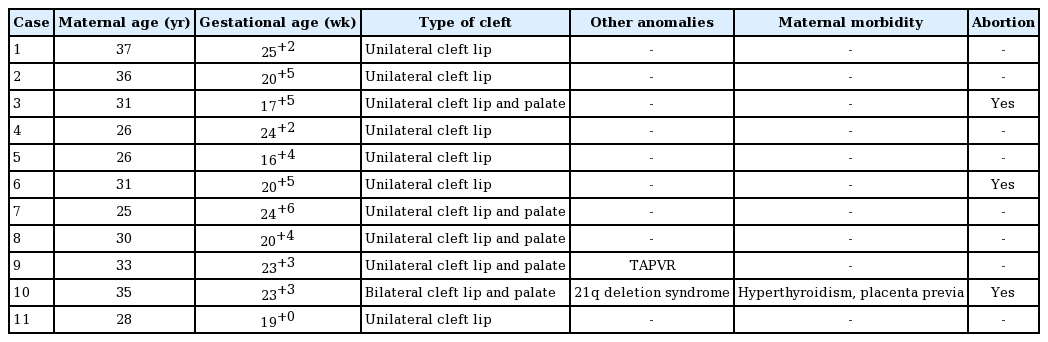
Patient data
The concordance rate of the sonographic and final diagnoses was 100% (8/8) (Table 2). Ten women reported that they were satisfied with the multidisciplinary management in our center (91%; very satisfied in nine cases, satisfied in one case, and no response in one case) (Table 3).
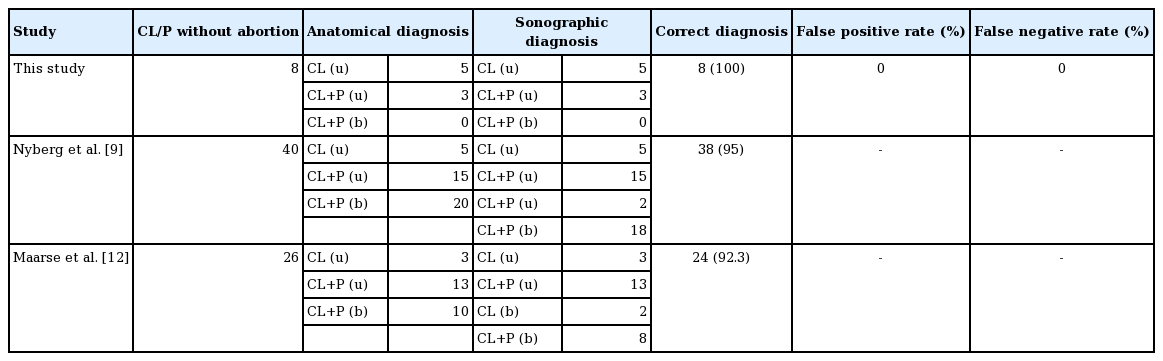
Accuracy of prenatal sonography
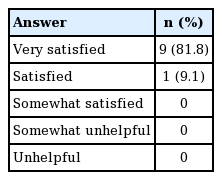
Patient satisfaction
Case 1 (No. 2)
Assessment of the fetal face during prenatal ultrasonography revealed cleft lip at 20+5 weeks. The parents were referred to the Congenital Disease Center, where they consulted with a plastic surgeon and an obstetrician. At birth, the infant had a unilateral complete cleft to the right of the philtrum with alveolar involvement. A nasoalveolar molding device with Grayson's method was inserted at the age of three weeks with alveolar approximation, and the nasal cartilage was not overstretched. The molding device was applied presurgically for approximately two months. After molding, rotation advancement cheiloplasty (Millard I method) was performed at the age of three months (Fig. 2).
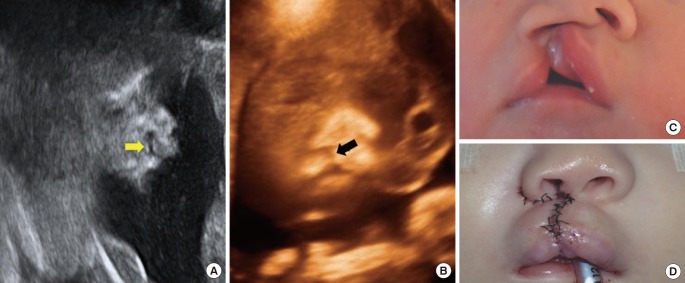
Case 1. Unilateral complete cleft lip
(A) Cleft lip of the fetal face (arrow) was seen on the prenatal ultrasonogram at 20+5 weeks. (B) Three-dimensional reconstruction. (C) At birth, the infant had unilateral complete cleft lip to the right of the philtrum. A nasoalveolar molding device with Grayson's method was inserted at the age of three weeks and applied for approximately two months. (D) Cheiloplasty was performed at the age of three months.
Case 2 (No. 6)
Left-sided cleft lip of the fetal face was detected on the prenatal ultrasonogram at 20+5 weeks. The mother was referred to the Congenital Disease Center, where she consulted with the cleft team. She showed a strongly negative attitude towards the fetal deformity and refused treatment with the goal of keeping the baby. Our team offered constant consultations with her and made every effort to persuade her to maintain the pregnancy, emphasizing the importance of life. Nevertheless, she abruptly stopped attending follow-up at our center. The fact that she aborted the fetus at another hospital was confirmed much later by telephone (Fig. 3).

Case 2. Unilateral complete cleft lip
Left-sided cleft lip of the fetal face (white arrows) was detect on the prenatal ultrasonogram at 20+5 weeks. The mother showed a strongly negative attitude towards the fetal deformity. She abruptly stopped attending follow-up at our center although our team offered extensive consultations and made every effort to persuade her to keep the pregnancy. The fact that she aborted the fetus at another hospital was confirmed much later by telephone.
DISCUSSION
The mother's fear of and feelings of repulsion towards a child with a birth defect is strong in almost every country. The rate of pro-choice opinions regarding artificial abortion if the fetus has an abnormality was found to be 54.1% in the US, 79.8% in the UK, 64.0% in Canada, and 77.4% in Japan [10]. Practically, legal artificial abortion in cases of fetal anomalies is allowed in more than 60% of the world [10]. In Korea, a national report from 2005 indicated that approximately 35% of respondents felt that artificial abortion due to a curable fetal abnormality was acceptable, and approximately 80% felt that it was justified in cases of an incurable fetal abnormality [10]. This indicates that many Korean parents would not readily accept a fetal deformity.
According to the artificial abortion-related legislation included in the Mother and Child Health Law in Korea, legal artificial abortion is allowed before the gestational age of 24 weeks in the following cases: the gravida or her spouse has a hereditary disorder that has a high risk of affecting the fetus, the gravida or her spouse has an infectious disease that has a high risk of affecting the fetus, conception by sexual assault, conception by incest, or if maintaining the pregnancy can severely harm the gravida [10]. No clause exists to permit artificial abortion due to of fetal CL/P in Korea. Artificial abortion is allowed without any restrictions of this type in the US, Canada, and most other countries in Europe. Among the Organization for Economic Cooperation and Development member countries, only Japan, Mexico, Korea, and Ireland have legal restrictions forbidding artificial abortion due to fetal abnormalities [10]. This indicates that many countries allow artificial abortion due to fetal anomalies and that feelings of repulsion towards abnormalities in offspring are strong worldwide. Thus, social and institutional care for the parent and fetus, especially if a fetal deformity is detected in a prenatal examination, is important for preventing illegal abortion in Korea. Such assistance can mitigate issues such as maternal health problems caused by illegal abortion by unlicensed practitioners.
In our Congenital Disease Center, 72% (8/11) of the women gave birth to babies who were diagnosed with CL/P during the prenatal ultrasound screening, and 28% (3/11) preferred an induced abortion. The calculated abortion rate was lower than expected, considering that 35% and 80% of respondents have been reported to be in favor of artificial abortion due to curable and incurable fetal abnormalities, respectively [10].
We propose that this slight decrease of the abortion rate occurred as a result of the help the parents received from the multidisciplinary management system at our center. Although the abortion rate was reported to be tenfold higher in cases with a prenatal diagnosis of CL/P in the Netherlands, Maarse et al. [7] and Davalbhakta and Hall [13] reported that 87% and 92% of women, respectively, gave birth to their babies despite a prenatal diagnosis of CL/P if they received prenatal counseling. Similarly to these studies, we found that a prenatal diagnosis of CL/P did not increase the artificial abortion rate in this study.
Prenatal counseling likely needs to begin early in order for the future parents to receive adequate information about the disability, including their duties and opportunities, the types of assistance they may receive from the community, the effects the disability will have on the quality of life of their babies, and to mentally prepare themselves [713]. Plastic surgeons can explain and discuss the anticipated disabilities and treatment plans according to the child's developmental stages.
We believe that this approach may prevent parents from being influenced by incorrect information received from untrustworthy sources and strengthen the attachment between the mothers and their babies. These are likely to be the decisive factors in lowering the abortion rate. Davalbhakta and Hall [13] proposed that parents would be less psychologically traumatized by the prenatal perception of CL/P of their babies than by its postnatal detection. Lippman [14] reported relieving parents' feelings of guilt during prenatal counseling by informing them that CL/P has a multifactorial background and that the etiology is not yet known.
Concerns exist that the prenatal diagnosis of cleft deformity will increase the abortion rate [1516171819]. Blumenfeld et al. [20] reported that 93.3% of women who tested positive for isolated fetal cleft lip in a prenatal ultrasound screening decided to terminate their pregnancy. This rate is much higher than the rate of 28% (3/11) achieved in our Congenital Disease Center [7]. Prenatal counseling by professionals and multidisciplinary team support of the parents could have been responsible for this difference.
Our study had several limitations. First, the sample number was very small, and further larger prospective randomized studies are required to generalize these results. However, even with a small sample size, the relatively high satisfaction rate shows the efficacy of multidisciplinary management. Second, although artificial abortion due to CL/P alone is illegal, the cases of abortion in our study were reported. These patients refused multidisciplinary treatment for keeping the baby with a congenital deformity at our center. If they expressed such an opinion, the Department of Obstetrics offered extensive consultation and exerted considerable effort to persuade them to maintain the pregnancy. Nevertheless, it was difficult from a practical point of view to remain involved in the case management of patients who emphatically refused treatment and left our institution. It was only possible for us to confirm whether an abortion was performed a considerable amount of time later. Finally, all cases in our study had CL or CL+P, with no cases of isolated CP. The prevalence of isolated CP is approximately one per 2,000 births. Isolated CP can be identified by using specialized two- and three-dimensional sonography after the gestational age of 20 weeks. The detection rate is low (about 34% and 1.4%), especially in cases in which it was restricted to only the soft palate [21]. Therefore, the high false negative rate should be explained to the parents. If a baby is born with CP, the baby and parent should be treated appropriately, with a similar multidisciplinary approach. In addition, a study of CL/P showed that the official prenatal ultrasonography findings were inconsistent with the actual facial structure identified after birth [22]. Sufficient explanation and consulting is needed in these rare cases.
We wish to emphasize the benefits of a multidisciplinary team approach to the systemic management of mothers and their CL/P babies. If the mother of an affected fetus is referred to a multidisciplinary team composed of obstetricians, plastic and reconstructive surgeons, pediatricians, and psychiatrists, she will undergo amniocentesis to detect the presence of associated abnormalities and will receive support and psychological counseling to relieve her feelings of guilt and to regain psychological stability. Thus, both the doctors and the future parents can prepare for the care of these babies. For these reasons, although a child with a birth defect is unlikely to be received well, the women whose fetuses were diagnosed with CL/P on prenatal ultrasound screening and who underwent multidisciplinary team management were more likely to decide to continue their pregnancy than would have been expected.
Notes
No potential conflict of interest relevant to this article was reported.