Inconspicuous Nasoethmoidal Encephalocele Might Be Wrongly Diagnosed
Article information
Dear Editor-in-Chief,
We have read the paper of Song et al. [1] on frontonasal dysplasia deformity. It was an interesting discussion of an image that depicts a boy with a nose deformity, and it was reported that no basal encephalocele was observed. We would like to point out that we had a similar case of a girl with the same nose deformity. As in the report by Song et al., our patient also presented with mild hypertelorism, a broad nasal root and a bifid nasal tip (Fig. 1). The defect at the nasal dorsum had never increased in size and was not cystic. Her parents were anxious about the cosmetic appearance of their child and requested an early excision of the nasal defect and rhinoplasty.

(A, B) A 6 months old, Malay girl with features of nasoethmoidal encephalomeningocele, including telecanthus, broadening of the nasal root with irregular nasal dorsal skin and lack of a nasal tip.
Intraoperatively, we noted a very small stalk passing between the nasal bone and the upper lateral cartilage (Fig. 2A, B). The stalk was faintly seen on the magnetic resonance imaging due to its very small size. This small stalk passed from an internal location between the frontal and ethmoidal bone to an external location between the nasal bone and the upper lateral cartilage (Fig. 2C).
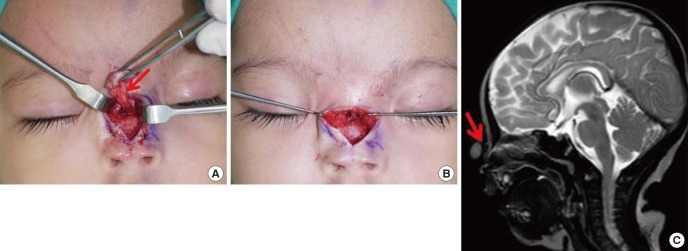
(A, B) Stalk of the lesion passing in between the nasal bone and upper lateral cartilage. (C) Small fine stalk in a T2-weighted magnetic resonance imaging (shown with a red arrow).
Due to this inconspicuous finding, a frontoethmoidal encephalocele may be missed and wrongly diagnosed. Frontoethmoidal encephalomeningocele is associated with hypertelorism, a broad nasal root, bifid nasal tip, widow's peak and encephalocele, all of which were present in our patient. Based on the clinical review by Rojvachiranonda et al. [2], our patient did have a small herniation mass with a very small stalk of 2 mm passing through a long narrow exit pathway. Due to the small diameter of the stalk and mass, there were no external bone defects or a huge facial deformity. Only skin thickening was present, without a secondary pressure effect, which correlates with the classification on the basis of the soft tissue aspect by Rojvachiranonda et al. [2]. Based on the proposed classification by Rojvachiranonda et al. [2], which describes a facial deformity, external bone defect, exit pathway and malformation of the brain, this patient could be classified as F1c E1NE E1 M0.
Thank you.
Yours sincerely,
Notes
No potential conflict of interest relevant to this article was reported.