Sebaceous Carcinoma Arising from the Nevus Sebaceous
Article information
Nevus sebaceous appears at birth or within several months after birth. Secondarily to nevus sebaceous, benign or malignant tumors might occur. Basal cell carcinoma has been reported to be one of the most common malignancies. Moreover, trichoblastoma, syringocystadenoma papilliferum, apocrine cystadenoma, squamous cell carcinoma, sebaceous epithelioma, and sebaceous carcinoma might also occur [1]. In particular, there are extremely rare cases in which sebaceous carcinoma occurs secondarily to the nevus sebaceous. That is, only four Korean cases and nine from overseas countries have been reported in the literature [2]. The authors describe a case of sebaceous carcinoma that arose from the nevus sebaceous of the scalp in a 33-year-old woman.
A 33-year-old woman visited us with a chief complaint of a 2×2 cm asymptomatic mass in the occiput. On past history, the patient had had a hairless yellowish plaque in the occiput since birth. Three months before the outpatient visit, the erythematous mass had begun to gradually grow in the lower 1/3 of the plaque (Fig. 1). The patient had no underlying diseases, nor did the patient have any notable findings from the family history. We performed a punch biopsy for both the yellowish plaque and the erythematous mass. This showed that the yellowish plaque was a nevus sebaceous and the erythematous mass was sebaceous epithelioma. It became evident, however, that it would be necessary to make a differential diagnosis from basal cell carcinoma originating from the sebaceous gland.

Preoperative view. A papillary erythematous mass of nevus sebaceous on the scalp.
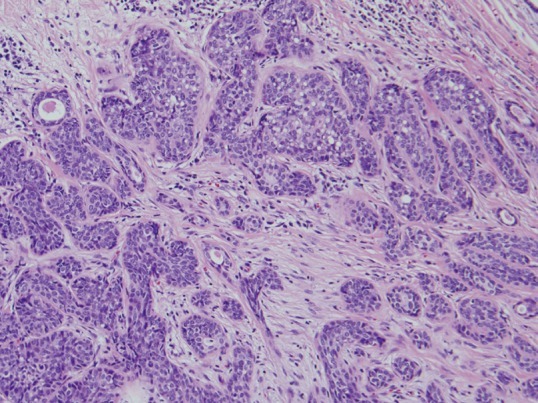
In the erythematous mass containing the nevus sebaceous, a wide excision was performed with a safety margin of 5 mm. A frozen section biopsy showed that there were no tumor cells on the resection margin. Following the resection, scalp defects of 2.5×5.0 cm in size remained (Fig. 2). The defects were reconstructed using a scalp rotational flap and primary closure (Fig. 3). A histopathologic examination of the resected erythematous mass was performed, and it revealed the presence of irregular lobules of varying size with a well-defined margin from the adjacent interstitial tissue in the dermis. In the center of each lobule, there were non-typical cells with a foamy cytoplasm and undifferentiated cells. This was indicative of typical sebaceous carcinoma (Fig. 4). Besides, this was also accompanied by the multiple presence of sebaceous epithelioma that comprises undifferentiated basaloid cells and mature sebocytes (Fig. 5).

Intraoperative view. Wide excision involving a 5-mm safety margin. Three separate rotation flaps equally positioned around the defect, raised and pivoted in the same direction.

Postoperative view. The reconstruction of the defect using a rotational flap and primary closure.

Histopathologic findings of sebaceous carcinoma. The tumor showing irregular lobules, infiltrating the surrounding tissue, composed of irregular pleomorphic basophilic cells with a foamy cytoplasm in the center of the lobule (black arrows) and undifferentiated cells with atypical mitotic features (black arrowhead) (H&E, ×200).
Histopathologic findings of sebaceous epithelioma. The tumor, showing the presence of multiple undifferentiated basaloid cells together with a potential to differentiate into sebaceous cells within an eosinophilic stroma (H&E, ×200).
The current case is a relatively young patient who presented with both benign and malignant tumors, showing sebaceous differentiation, as well as the nevus sebaceous. The patient was tentatively diagnosed with Muir-Torre syndrome. A gastrofiberscopy, a colonofiberscopy, and an abdominopelvic computed tomography were therefore performed to search for gastrointestinal and urologic tumors, but no underlying malignancies were found. The patient was followed for 2 years after the operation with no recurrent episodes and no occurrence of internal malignancies.
Sebaceous carcinoma is a rare malignant tumor that is differentiated from the epithelium lining of the sebaceous gland [2]. Depending on the sites of occurrence, it is classified into ocular sebaceous carcinoma and extraocular sebaceous carcinoma. Ocular sebaceous carcinoma accounts for 75% of total cases, and it also accounts for 1% to 5.5% of total cases of eyelid malignancies [3]. The remaining 25% occur at extraocular sites. However, according to the largest study of sebaceous carcinoma in a United States population [4], the proportion of ocular sebaceous carcinoma was 38.7% and the mean age of onset was 72-year-old. In the current case, the patient was 33 years old, and this is a relatively young age. To our knowledge, this is the youngest case of extraocular sebaceous carcinoma that has been reported up to the present in Korea.
Muir-Torre syndrome is a rare autosomal dominant genetic trait. This is characterized by the presence of more than one of the following: a sebaceous gland tumor, i.e., sebaceous adenoma, sebaceous epithelioma, or sebaceous carcinoma. It is also accompanied by internal malignancies. Of the possible internal malignancies, the most common one is colorectal cancer. This is followed by genitourinary cancer [5]. It would therefore be desirable to consider the possibility of Muir-Torre syndrome and to perform the clinical and laboratory examinations for internal malignancies in patients who are diagnosed with sebaceous carcinoma. Also in the current case, the patient presented with benign and malignant tumors arising from the sebaceous gland at a younger age. This led to an impression of Muir-Torre syndrome followed by various clinical and laboratory examinations. However, there were no other internal malignancies. In patients with Muir-Torre syndrome, however, the sebaceous gland tumor might occur prior to or following the occurrence of internal malignancies. Otherwise, it might also be concurrently present with them. Accordingly in the current case, regular check-ups are being performed regularly to monitor the recurrence of sebaceous carcinoma and the occurrence of internal malignancies.
The general treatment guidelines are that a wide excision with a safety margin of 5 to 6 mm should be performed in combination with a frozen section biopsy and a permanent section one [1,3]. In the current case, a wide excision was performed with a safety margin of 5 mm. Synchronously, a frozen section biopsy was performed for the resection margin.
The ocular sebaceous carcinoma had a metastasis to such organs in 3% to 25% of total cases, based on which a poor prognosis has been well documented [2,3]. The doctor should ask about family history of skin and internal malignancies. A physical examination and laboratory examinations should be performed as well as palpation of the lymph nodes and adjacent and contiguous structures to determine the extent of disease.
The authors experienced a very rare case of extraocular sebaceous carcinoma that occurred in the nevus sebaceous of the occiput, and have obtained good treatment outcomes using a wide excision with a safety margin of 5 mm and a local flap on a frozen section biopsy. Here, we report our case with a review of the literature.
Notes
No potential conflict of interest relevant to this article was reported.