A Rare Case of Bilateral Upper Extremity Hypercalcinosis in Systemic Sclerosis Requiring Multiple Radical Debridements
Article information
Systemic sclerosis is an autoimmune connective tissue disease that may affect the hands [1]. Hypercalcinosis in systemic sclerosis is a rare and poorly defined entity characterized by widely metastatic benign calcific deposits [2]. We describe a case of bilateral upper extremity hypercalcinosis requiring multiple radical debridements, in which local tissue rearrangement was used for sequential successful reconstructions.
The patient was a 56-year-old woman with a history of systemic sclerosis. She presented to a hand surgeon with two severely painful calcific lesions of her left thumb pulp and a large area of calcinosis on the extensor surface of the right elbow after failed medical treatment. She subsequently underwent excision and curettage of the left thumb and right elbow lesions with local tissue rearrangement of all defects.
The patient remained pain-free for 26 months and then presented with painful calcific lesions of the right posterior forearm and right index finger. She underwent radical excision of a 3 cm×15 cm lesion of the forearm with local tissue rearrangement and excision of a 1-cm right index finger lesion.
Three months after the second operation, the patient experienced recurrent painful calcinosis of the right index finger and left thumb along with new calcinosis of the right thumb (Fig. 1). These lesions were excised and, 20 months later, she returned with recurrent painful lesions of the left thumb and right index finger and new lesions of the right ring finger. She underwent radical debridement of all lesions (Fig. 2). Overall, her postoperative courses were uncomplicated, requiring only local wound care for poor wound healing. At 8.5 months of follow-up, she again developed recurrence of painful calcific deposits (Fig. 3).

Plain radiograph demonstrating soft tissue calcification in the volar aspect of the distal thumb at the level of the distal phalanx and at the head of the proximal phalanx with acro-osteolysis of the distal phalanx.
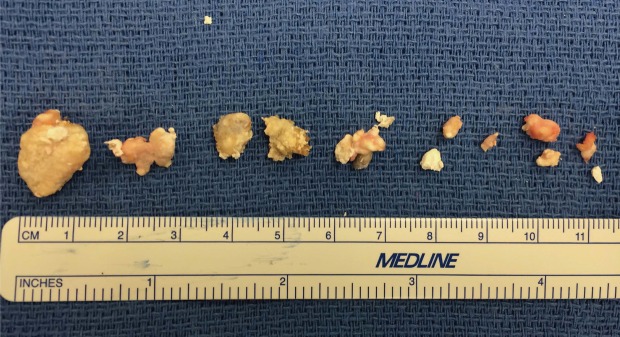
Calcific deposits after radical debridement of the left thumb and right index and ring fingers; the patient's fourth such radical debridement.

Postoperative photographs of the right and left hands 8.5 months after the radical debridement of calcific deposits in the left thumb and right index and ring finger, with evidence of recurrence.
Hypercalcinosis is a severe and proliferative form of calcinosis seen in systemic sclerosis and calcinosis, Raynaud phenomenon, esophageal dysmobility, sclerodactyly, and telangiectasia syndrome, resulting in widely metastatic deposits that may become painful, ulcerated, or infected [2]. Hand involvement in this disease process is common and is frequently the first manifestation of disease [1]. We present a patient with bilateral upper extremity hypercalcinosis diagnosed both clinically and radiographically. The major indication for surgery in this case was severe pain, which we hypothesize was due to a compartment syndrome-like effect of the calcium within the small areas of the digit.
Various options have been described for the treatment of hand lesions, but radical debridement was performed in each operation in this patient [34]. The time to recurrence ranged from three to 26 months in this case, highlighting the aggressive nature of this case of hypercalcinosis. While the full armamentarium of local and distant hand flaps is available for reconstruction, we recommend local tissue rearrangement allowing for the possibility of re-advancement, similar to the principle of pressure sore reconstruction, due to the high likelihood of lesion recurrence.
Notes
No potential conflict of interest relevant to this article was reported.