Wrist Pain due to Abnormal Extensor Carpi Ulnaris Tendon
Article information
Pain arising from lesions in the extensor carpi ulnaris (ECU) is known to occur mainly due to tenosynovitis, tendon rupture, and subluxation or dislocation of the ECU tendon [12]. However, anomalies of the ECU tendon itself and the surrounding extensor retinaculum are also possible factors contributing to the impairment of function at the dorso-ulnar aspect of the wrist and little finger [23]. We report a case in which an abnormal ECU tendon slip was revealed during exploration of the wrist.
A 28-year-old right-handed female neurosurgeon visited our clinic due to dorso-ulnar wrist pain in her dominant hand for six months. The pain was exacerbated during wrist motion, especially during forearm supination for handling the needle holders in the operating field. A physical examination revealed no sensory changes and no specific signs, including the Phalen and Finkelstein tests. Radiographic studies also showed no problems such as joint subluxation. The hand showed a slight tender swelling of the ECU tendon around the wrist. With the suspicion of tenosynovitis, steroid injection into the sixth compartment was performed. However, the pain did not respond to medical treatment. Electrodiagnostic studies revealed no abnormalities. On exploration, we found the abnormal insertion of an additional ECU tendon slip into the radial inner side of the sixth compartment (Fig. 1). After simple excision of the entire abnormal ECU tendon slip, her symptoms improved.
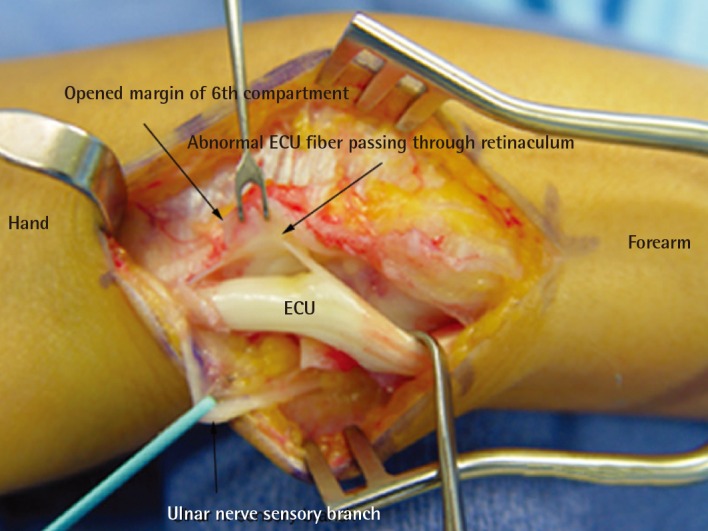
The abnormal insertion of an additional extensor carpi ulnaris (ECU) tendon slip into the radial inner side of the sixth compartment.
The ECU tendon is enclosed in the sixth compartment of the extensor retinaculum and various anomalies of the ECU tendon have been reported [23]. The prevalence of an accessory tendinous slip arising from the ECU tendon has been reported to be 10% to 34% [24], and Barfred and Adamsen [3] noted that the accessory tendinous slip of the ECU was sometimes connected with the extensor digiti minimi. Nakashima classified accessory slips into three types according to the insertion point of the main tendon to the fifth metacarpal bone: type A, on the base along with the main tendon; type B, on the midsection; and type C, on the head [2]. The case presented here belonged to type A. The average width of the slips has been reported to range from 1–1.53 mm [23], while the presented case showed a slip 1.5 mm in width and 2 cm in length. Taleisnik et al. [5] observed that the transverse fibers of the medial wall of the sixth compartment extend proximally to become confluent with the epimysium of the ECU, and are reinforced by the linea jugata, which normally prevents ECU tendon subluxation during full supination. Since the ECU tendon is exposed to maximal traction when the forearm is supinated, we believe that her wrist pain was induced by repetitive and excessive supination-pronation activity, which might otherwise remain non-symptomatic given usual movement patterns. Anatomical variations of the ECU may affect diagnostic and surgical procedures involving the dorso-ulnar aspect of the wrist. During surgery performed on the ECU, the surgeon must be aware of the possible existence of an accessory tendinous slip that may cause ECU lesions to persist.
Notes
No potential conflict of interest relevant to this article was reported.