Delayed Foreign Body Reaction Caused by Bioabsorbable Plates Used for Maxillofacial Fractures
Article information
Abstract
Background
Bioabsorbable plates and screws are commonly used to reduce maxillofacial bones, particularly in pediatric patients because they degrade completely without complications after bone healing. In this study, we encountered eight cases of a delayed foreign body reaction after surgical fixation with bioabsorbable plates and screws.
Methods
A total of 234 patients with a maxillofacial fracture underwent surgical treatment from March 2006 to October 2013, in which rigid fixation was achieved with the Inion CPS (Inion, Tampere, Finland) plating system in 173 patients and Rapidsorb (Synthes, West Chester, PA, USA) in 61 patients. Their mean age was 35.2 years (range, 15-84 years). Most patients were stabilized with two- or three-point fixation at the frontozygomatic suture, infraorbital rim, and anterior wall of the maxilla.
Results
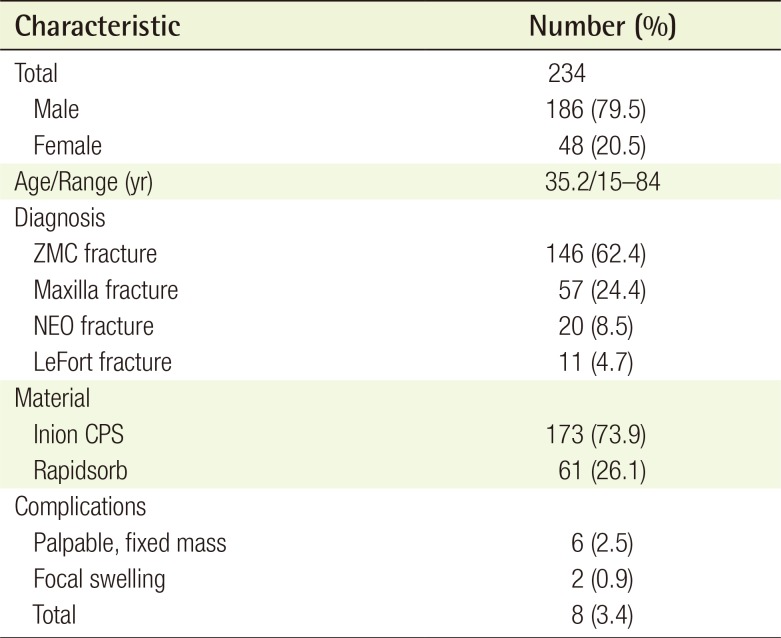
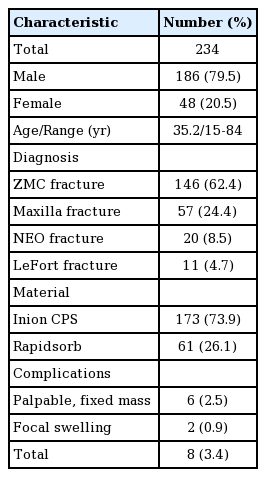
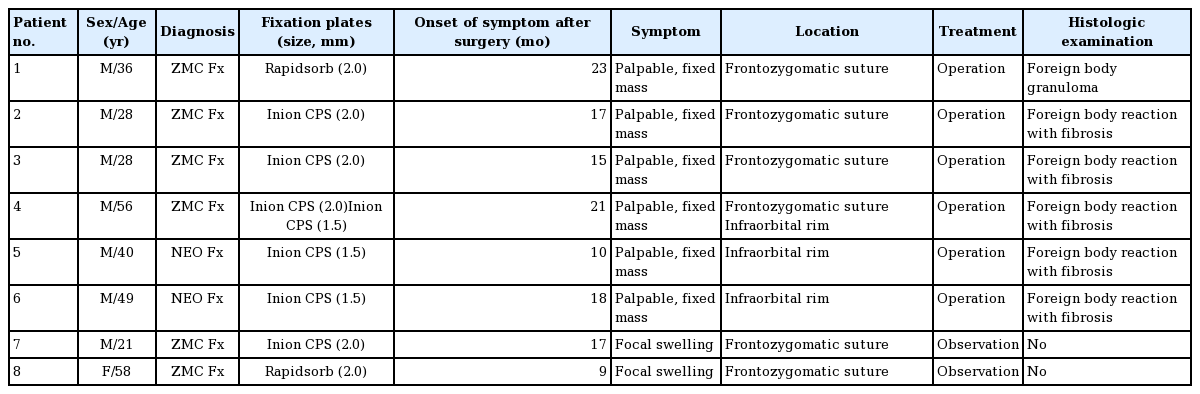
Complications occurred in eight (3.4%) of 234 patients, including palpable, fixed masses in six patients and focal swelling in two patients. The period from surgical fixation to the onset of symptoms was 9-23 months. Six patients with a mass underwent secondary surgery for mass removal. The masses contained fibrous tissue with a yellow, grainy, cloudy fluid and remnants of an incompletely degraded bioabsorbable plate and screws. Their histological findings demonstrated a foreign body reaction.
Conclusions
Inadequate degradation of bioabsorbable plates caused a delayed inflammatory foreign body reaction requiring secondary surgery. Therefore, it is prudent to consider the possibility of delayed complications when using bioabsorbable plates and surgeons must conduct longer and closer follow-up observations.
INTRODUCTION
Metallic plates and screws are commonly used for rigid internal fixation during maxillofacial surgery [1]. However, metallic implants have problems, such as visibility on radiography, palpability, bone erosion and growth restrictions, thermal sensitivity, and the need for removal [23]. Various bioabsorbable materials have been developed to overcome these disadvantages of metallic implants [4]. Ideally, bioabsorbable plates are sufficiently rigid and biocompatible, provide sufficient stability to allow bone healing, and are eliminated completely after osteosynthesis without a foreign body reaction [56]. They do not require any secondary operation for removal due to their characteristics. Thus, bioabsorbable plates and screws are commonly used to reduce maxillofacial bones, particularly in pediatric patients [7]. Polyglycolic acid (PGA) and polylactic acid (PLA) are the polymers used most widely to manufacture bioabsorbable plates and screws [58]. Plate degradation properties and rates vary depending on the ratio of lactic acid isomers or glycolic acid. If the bioabsorbable plates fail to degrade completely or undergo polymeric breakdown beyond the maximum metabolic clearance rate, the remnant material can become a nidus for an inflammatory foreign body reaction [8910]. Copolymers such as polylactic-co-glycolic acid are often used commercially because these complications are almost always associated with homopolymers [81011]. Many studies have reported the efficacy and clinical utility of bioabsorbable plates, but few reports are available on complications associated with the plates, resulting from inadequate degradation of the plates [1213]. Between March 2005 and October 2013, we encountered eight cases of a delayed foreign body reaction after surgical fixation with bioabsorbable plates and screws. We report these cases with a review of the literature.
METHODS
The medical records of 372 patients who underwent surgical treatment with metal plates (n=138), bioabsorbable plates (n=176), or both (n=58) for a maxillofacial fracture between March 2006 and October 2013 were reviewed retrospectively. The data included fracture patterns, fixation methods/materials, and any complications. A total of 234 patients who were treated using bioabsorbable plates (186 men and 48 women; age, 15-84 years; mean age, 35.2 years) were included in our study. They were diagnosed with a zygomaticomaxillary complex fracture (n=146), maxilla fracture (n=57), nasoethmoid orbital fracture (n=20), or a LeFort fracture (n=11). Rigid fixation was achieved with the Inion CPS (Inion, Tampere, Finland) plating system in 173 patients and Rapidsorb (Synthes, West Chester, PA, USA) in 61 patients (Table 1). Metal plates were used with bioabsorbable plates in 58 of 234 patients. Patients were selected to receive bioabsorbable fixation on the basis of the degree of bony displacement, fracture pattern or location, and patient age. Patients with an isolated, noncomminuted, minimally displaced fracture were good candidates for bioabsorbable fixation. However, biodegradable plates were regarded as the most appropriate in young patients irrespective of the fracture type. All fractures were approached in the standard fashion, and most patients were stabilized with a two- or three-point fixation at the frontozygomatic suture (2.0-mm plate and 7-mm screws), infraorbital rim (1.5-mm plate and 6-mm screws), and anterior wall of the maxilla (1.5-mm mesh plate and 4-mm screws).
Patient demographics
In the statistical evaluation, a logistic regression analysis was used (level of significance, P<0.05). Odds ratios were calculated, and 95% confidence intervals were constructed where appropriate.
RESULTS
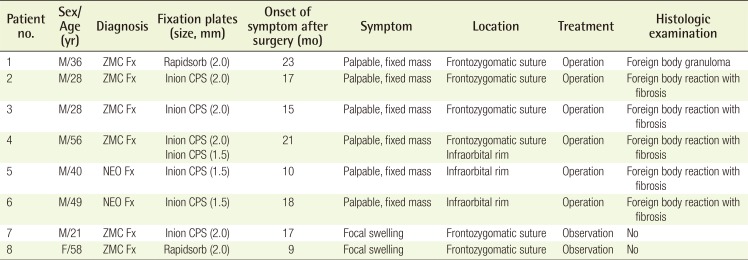
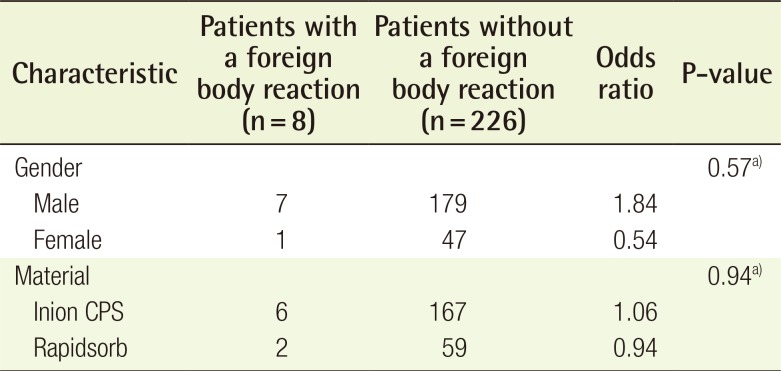
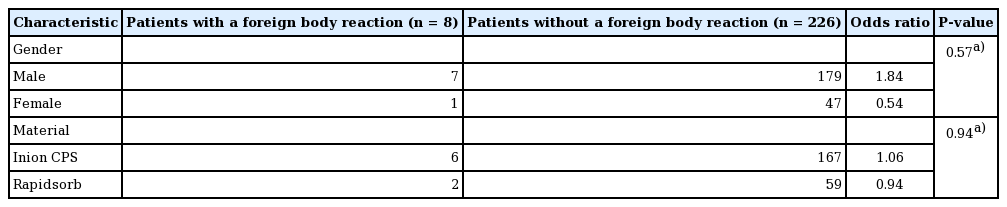
A total of 234 patients achieved satisfactory bone healing with favorable restoration in form and function and no signs of inflammation, such as a heating sensation or tenderness, during the early postoperative period. Complications occurred in eight (3.4%) of the 234 patients, including palpable, fixed masses in six patients and focal swelling in two patients (Table 1). Six patients were diagnosed with a zygomaticomaxillary complex fracture, and two were diagnosed with a nasoethmoid orbital fracture. Six of them were fixed with Inion CPS plates, and two were fixed with Rapidsorb plates. The period from surgical fixation to the onset of symptoms was 9-23 months. We were determined to perform the operations when the masses formed. Two patients with focal swelling were under observation without surgery for a mean duration of 13 months after fixation. Six patients with a mass underwent secondary surgery for the exploration and removal of the mass at a mean duration of 17.7 months after fixation. The masses developed in the bioabsorbable fixation sites, including the frontozygomatic suture (n=3), the infraorbital rim (n=2), or both (n=1) (Table 2). A surgical skin incision was made along the previous scar. The masses contained fibrous tissue with a yellow, grainy, and cloudy fluid and remnants of incomplete degraded bioabsorbable plates and screws. A connective tissue capsule was seen around the foreign material and was composed of thin collagen fibers with numerous fibroblasts and fibrocytes. Multinucleate giant cells, lymphocytes, and histiocytes were evident. The masses were diagnosed as a foreign body reaction. The tissue culture results were negative in all patients, and the masses did not recur during a 1-year follow-up after recovery. There was no difference in gender and material type causing the foreign body reaction between the patients with and those without a foreign body reaction (Table 3).
Characteristics of the patients with complications
Odds ratio of patients with and those without a foreign body reaction
Case 1 (patient no. 1)
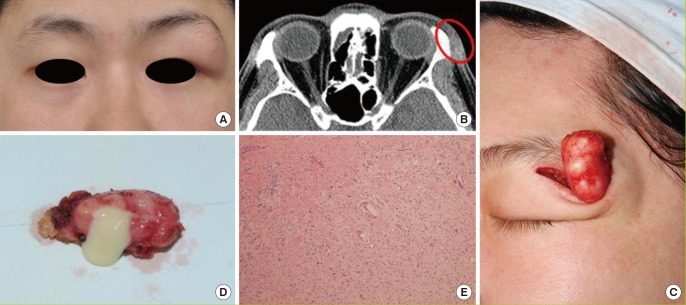
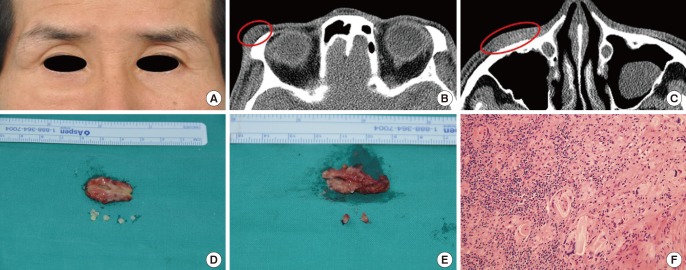
A 36-year-old man visited our clinic to treat a mass on the left frontozygomatic suture. He had fallen 29 months earlier, under alcohol intoxication. The patient had a left zygomaticomaxillary complex fracture, which was fixed with a Rapidsorb 2.0-mm 4-hole plate on the frontozygomatic suture, a 1.5-mm 8-hole plate on the infraorbital rim, and a bioabsorbable mesh plate on the anterior wall of the maxilla. He suffered from a palpable, fixed mass measuring 1 cm×2 cm for 6 months (Fig. 1A). A computed tomography (CT) scan 23 months after surgery showed soft tissue thickening on the left frontozygomatic suture (Fig. 1B). The patient had secondary surgery for the exploration and removal of the mass. The resected mass contained chronic inflammatory tissue with a grainy, cloudy liquid, and no gross evidence of a plate or screws inside the mass (Fig. 1C, D). However, the histological findings of the mass revealed the fine fragments of a foreign body with inflammatory cell infiltration, which was diagnosed as a foreign body granuloma (Fig. 1E).
Case 1 (patient no. 1)
(A) Preoperative clinical view 29 months after Rapidsorb plate fixation. (B) Computed tomography scan shows soft tissue thickening on the left frontozygomatic suture (red circle). (C) Fibrous encapsulated mass. (D) Resected mass containing inflammatory tissue with a yellow, cloudy liquid. (E) Fine foreign body fragments, multinucleated giant cells, lymphocytes, and histiocytes are seen (H&E, ×100).
Case 2 (patient no. 2)
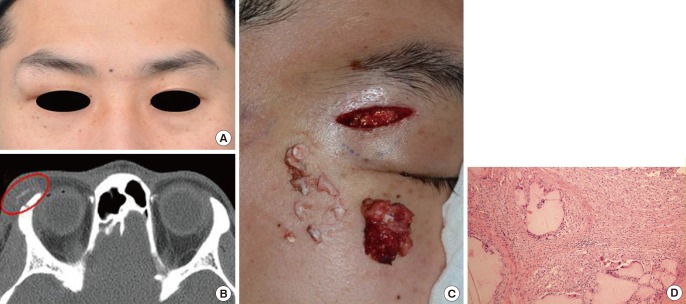
A 28-year-old man was struck on the right side of the face while snowboarding. The patient had a right zygomaticomaxillary complex fracture, which was fixed with the Inion CPS 2.0-mm 4-hole bioabsorbable plate on the frontozygomatic suture, a 1.5-mm C-shaped 7-hole plate on the infraorbital rim, and a bioabsorbable mesh plate on the anterior wall of the maxilla. The patient visited our outpatient clinic 17 months later complaining of a palpable mass, measuring 3 cm×2 cm, on the left frontozygomatic suture (Fig. 2A). The mass was a painless, visible, fixed mass. A CT scan showed a high-density content mass on the right frontozygomatic suture (Fig. 2B). The patient underwent secondary surgery for the exploration and removal of the mass. The bioabsorbable plate and screws had been replaced by a fibrous capsule, which contained a yellow, cloudy fluid and the remnants of the incompletely degraded bioabsorbable plate and screws (Fig. 2C). The histological findings of the mass showed a foreign body reaction with fibrosis (Fig. 2D).
Case 2 (patient no. 2)
(A) Preoperative clinical view 17 months after Inion CPS plate fixation. (B) Computed tomography scan showing high-density content with soft tissue thickening on the right frontozygomatic suture (red circle). (C) Resected mass containing a yellow, cloudy fluid and the remnants of an incompletely degraded bioabsorbable plate and screws. (D) Foreign body material with multinucleated giant cells, fibroblasts, lymphocytes, and histiocytes (H&E, ×100).
Case 3 (patient no. 4)
A 56-year-old man visited our clinic to receive treatment for a mass on the right frontozygomatic suture and infraorbital rim (Fig. 3A). He had fallen while driving a concrete mixer truck 25 months earlier. The patient had a right zygomaticomaxillary complex fracture, which was fixed with the Inion CPS 2.0-mm 4-hole plate on the frontozygomatic suture and the 1.5-mm 6-hole plate on the infraorbital rim. He suffered from two palpable, fixed masses, measuring 2.5 cm×1 cm each, for 4 months. A CT scan showed soft tissue thickening on the right frontozygomatic suture and infraorbital rim (Fig. 3B, C). The patient underwent secondary surgery for the exploration and removal of the mass. The mass contained fibrous tissue with a yellow, cloudy fluid and the remnants of the incompletely degraded bioabsorbable plate and screws (Fig. 3D, E). The histological findings of the mass demonstrated a foreign body reaction with fibrosis (Fig. 3F).
Case 3 (patient no. 4)
(A) Preoperative clinical view 25 months after Inion CPS plate fixation. (B) Computed tomography scan shows soft tissue thickening on the right frontozygomatic suture (red circle). (C) Soft tissue thickening on the right infraorbital rim (red circle). (D) Resected mass containing a yellow, cloudy fluid and remnants of an incompletely degraded bioabsorbable plate and screws on the right frontozygomatic suture. (E) Resected mass on the right infraorbital rim. (F) Foreign body material with multinucleated giant cells, fibroblasts, lymphocytes, and histiocytes (H&E, ×200).
DISCUSSION
Bioabsorbable plates ideally provide rigid fixation during the initial bone healing phase and are degraded by the body after osteosynthesis. In addition, these plates must be biocompatible with the recipient environment to prevent a significant inflammatory foreign body reaction [56]. Multiple factors, such as the chemical composition, size, and shape of bioabsorbable plates, affect the occurrence of foreign body reactions [8]. The results of several studies reveal that the foreign body reaction of a bioabsorbable plate results from an inadequate degradation of the chemical components of the plate. PGA and PLA are popular among several chemical compositions for bioabsorbable plates, and PLA exists in two different isomeric configurations of poly-L-lactic acid (PLLA) and poly-DL-lactic acid (PDLLA) [58]. PGA and PLA biodegradation occurs in a two-stage process. The first stage relies on the hydrolysis of the polymer's chemical bonds, thereby creating a shorter-chain molecule. The presence of these small polymer fragments can evoke a foreign body reaction. Then, they are phagocytized by macrophages and carried to the liver for metabolism. In the second metabolic phase, the breakdown products are metabolized to CO2 and H2O [5681014]. Secondary surgery for removal can be avoided through this process. Degradation properties and rates differ according to the main chemical components because they depend on the crystallinity and hydrophobicity of the polymers. PGA is a hard crystalline polymer and is less hydrophobic, so it undergoes rapid breakdown within 1 year. In contrast, PLA is a semicrystalline polymer and is highly hydrophobic, so it is degraded much more slowly within 5-6 years. Therefore, PGA is typically used in conjunction with PLA to create better strength and degradation profiles than those of either of the homopolymers alone [81011]. The Rapidsorb plate is manufactured from 85:15 poly (L-lactide-co-glycolide, PLGA). This copolymer is formed by combining PLLA and PGA. These plates maintain approximately 85% of their initial strength after 8 weeks and are completely absorbed after 1 year [15]. The Inion CPS plate is a copolymer of PLLA, PLDLA, and trimethylene carbonate. These plates are absorbed slowly, retaining 70% of their initial strength at 9 weeks, and they are completely degraded in 2-4 years [16].
In this study, six patients had palpable, visible masses and two patients had focal swelling around the bioabsorbable plates and screws. No risk factors of a foreign body reaction, namely gender and material type, could be found (Table 3). Most of the complications occurred in the frontozygomatic suture, which was fixed with a large-volume, 2.0-mm-thick bioabsorbable plate and 7-mm screws. As the implant materials have high volume and thickness, dead space may form and lead to fluid collection and a foreign body reaction [17]. In addition, this complication is caused by inadequate degradation, as degradation properties and rates are influenced by implant volume, geometrical shape, and chemical composition [18]. In contrast, there was no complication in the anterior wall of the maxilla. We think that this can be attributed to the small-volume implant, 1.5-mm mesh plate, and 4-mm screws used for fixation; further, the small polymer fragments derived from the first degradation process were partially absorbed into the maxillary sinus without a foreign body reaction.
The resected masses of six patients were diagnosed as foreign body reactions with fibrosis (n=5) and a foreign body granuloma (n=1). The patient with a foreign body granuloma was fixed with a 2.0-mm Rapidsorb plate. No gross evidence of a plate or screws was detected inside the granuloma, but fine foreign body fragments with inflammatory cell infiltration were seen histologically. This finding occurred because the Rapidsorb plate was almost absorbed 29 months after surgery. Two patients who were under observation without surgery continue to be monitored. Their symptoms improved to some degree, but mild focal swelling remains 6 years after surgery.
Plate degradation properties and rates change depending on the characteristics of the bioabsorbable plates, such as chemical composition and implant volume. Inadequate degradation can cause a delayed foreign body reaction with inflammation, thus requiring a second exploratory operation. In addition, a palpable mass or focal swelling resulting from a foreign body reaction can remain for years. Therefore, it is prudent to consider delayed complications when using bioabsorbable plates, and surgeons should conduct longer and closer follow-ups.
Notes
This article was presented as an E-Poster at the 72nd Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 7-9, 2014 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.