Kabuki Syndrome with Cleft Palate
Article information
Kabuki syndrome is a rare condition characterized by multiple congenital anomalies and intellectual disabilities [1]. The etiology of Kabuki syndrome is unclear, but the syndrome is known to have an autosomal dominant mode of inheritance. Furthermore, mutations in the MLL2 and KDM6A genes have recently been suggested as causes of this syndrome [2]. The five major clinical manifestations of this condition are distinctive facial features, skeletal anomalies, dermatoglyphic abnormalities, short stature, and intellectual disability.
Among these characteristics, the peculiar facial features that are common in all the patients presenting with Kabuki syndrome are the most striking and noticeable aspects of this syndrome. These include long palpebral fissures with lower lateral eyelid eversion, arched eyebrows with the lateral one-third dispersed or sparse, prominent ears, and a short columella with a depressed nasal tip. Because the facial appearance of a person with this syndrome resembles the makeup of Kabuki actors, this syndrome is called Kabuki syndrome.
Along with cardinal manifestations, many additional features have been reported. Among these anomalies, cleft palate is a common feature reported in about half of the patients with Kabuki syndrome [3]. However, thus far, only a few reports have discussed cleft palate in Kabuki syndrome patients. The aim of this study is to discuss the cases of five patients of Kabuki syndrome with cleft palate and describe their characteristic facial features.
Between March 2009 and February 2014, five patients (one boy and four girls) with cleft palate associated with Kabuki syndrome visited the plastic surgery clinic at our medical center. The age of the patients ranged from 10 months to 7 years. As shown in Figs. 1 and 2, all these patients had horizontally long palpebral fissures, eversion of the lower lateral eyelid, arched eyebrows with the lateral one-third dispersed, prominent ears, and a low nasal tip, which corresponded to the peculiar facial features of Kabuki syndrome. The patients were diagnosed with Kabuki syndrome on the basis of these facial features and the accompanying anomalies. All five patients presented with developmental delays and congenital heart disease: two patients had a congenital atrial septal defect and one of them underwent surgical correction. Another patient had a history of ventricular septal defects, and the other two had a combination of coarctation of the aorta and a ventricular septal defect, and they all underwent surgery. Other associated anomalies such as congenital scoliosis, diaphragmatic hernia, and multicystic dysplastic kidney were observed in one patient each. None of the patients underwent a genetic evaluation to determine whether there were any MLL2 or KDM6A gene mutations. One patient underwent a genetic test of the ELN gene to rule out Williams syndrome, but the result was negative.

Five-year-old girl with Kabuki syndrome. She underwent two-flap palatoplasty for incomplete cleft palate.
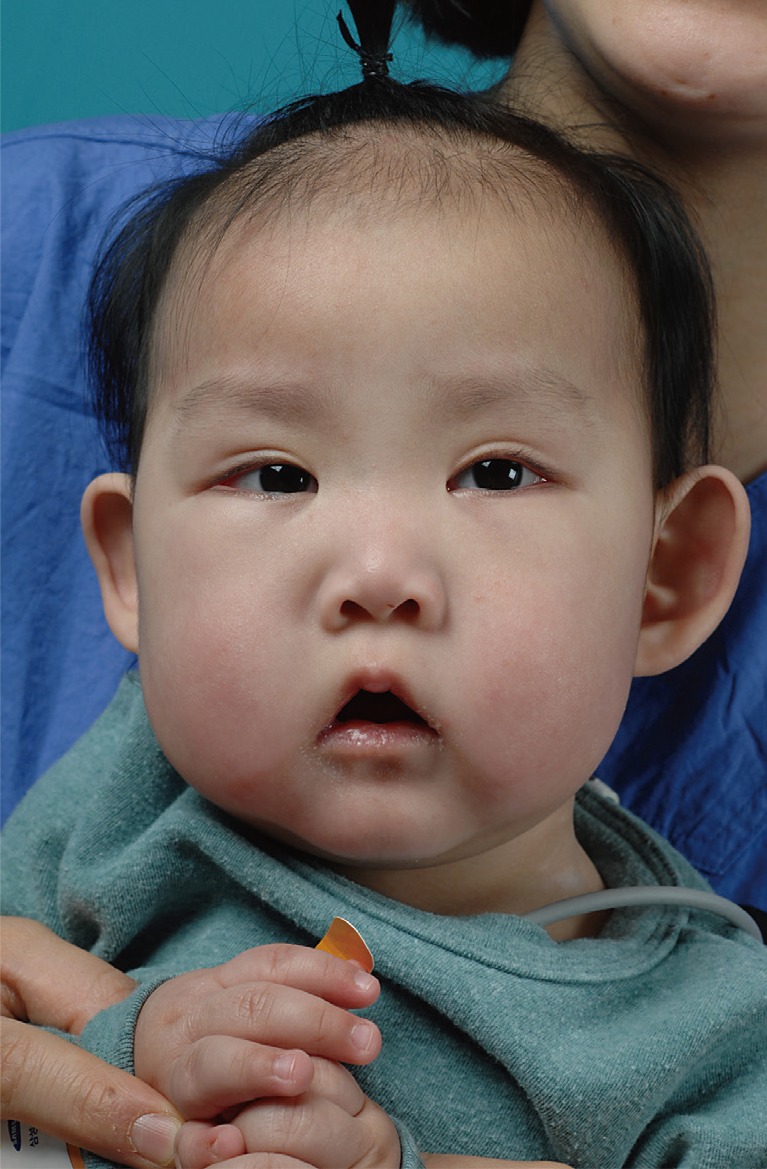
Twenty-month-old girl with Kabuki syndrome. She underwent two-flap palatoplasty for incomplete cleft palate.
Of these five patients, two of them presented with overt incomplete cleft palate and another two presented with submucous cleft palate. The other patient had a combination of submucous and incomplete-type cleft palate. All patients had a history of swallowing difficulty and frequent otitis media in infancy. In two of the patients who underwent palatoplasty when they were 20 months and 7 years old, overt hypernasality could be heard. Palatoplasty was performed in all five cases. Two-flap palatoplasty was performed in the incomplete cleft palate cases, and double opposing Z-plasty was performed in the submucous cleft palate cases and the combination of submucous and incomplete-type cleft palate case. No postoperative complication occurred in any of the patients, but one developed velopharyngeal insufficiency that could not be expected to improve by speech therapy, so the patient underwent pharyngeal flap surgery four years after palatoplasty.
Kabuki syndrome is a rare genetic disorder that has been estimated to occur in every 32,000 to 86,000 people. The characteristic facial features of this syndrome make typical cases highly recognizable. We could also easily observe the typical facial features of Kabuki syndrome in this series.
Apart from the typical facial gestalt, this syndrome has such diverse systemic clinical manifestations that include craniofacial abnormalities, such as cleft lip and palate; visceral manifestations, such as cardiac malformation and urogenital abnormalities; skeletal abnormalities, such as scoliosis and abnormalities of the fingers; and immune deficiency [4].
In this study, we reviewed the cases of five patients with Kabuki syndrome who presented with cleft palate. Previous studies observed isolated cleft palate in 50% to 69.7% of the patients and submucous cleft palate in 15.2% to 50% of the patients. Similar to a previous study, our study showed a high ratio of submucous cleft palate among patients having Kabuki syndrome with cleft palate [5]. It should be noted that submucous cleft palate, which can be easily misdiagnosed, should be routinely checked in patients with Kabuki syndrome, due to a high proportion of this population.
Cardiovascular anomalies are known to affect approximately 50% of the patients with Kabuki syndrome [4]. In contrast, a notable finding in this series is that every patient has a history of congenital cardiac defects with varying severity from a simple atrial septal defect that does not necessitate surgical intervention to a combination of multiple cardiac anomalies. This high ratio of cardiac manifestations in patients with Kabuki syndrome with cleft palate may be attributed to a small number of cases studied, and further genetic or molecular studies are necessary to reveal the relationship between different clinical manifestations.
In these five cases of Kabuki syndrome with cleft palate, the facial features are the key aspects that aid the diagnosis of this rare syndrome. In particular, cleft palate is not an unusual presentation in patients with Kabuki syndrome, accounting for up to 50% of the patients with Kabuki syndrome. It is important for pediatricians and plastic surgeons to always be aware of Kabuki syndrome when patients present peculiar and characteristic facial features of this syndrome, to rule out other associated anomalies including cleft palate.
Notes
No potential conflict of interest relevant to this article was reported.