Bilateral Dermoid Cysts on the Lateral Ends of Eyebrows
Article information
Dermoid cysts are a type of benign periorbital tumor that is frequently encountered in children. According to New and Erich, dermoid cysts originate from dermal and epidermal inclusions along the embryonic cleft closure lines located in the head and neck [1]. Periorbital involvement accounts for more than 50% of the pediatric cases of these cysts. Periorbital dermoid cysts usually manifest as painless, slow-growing swellings on the lateral eyebrows. Sometimes, they can cause inflammation and have a mass effect on the adjacent tissue or bone. Unilateral dermoid cysts on the lateral ends of eyebrows are common, but bilateral dermoid cysts are very rare and only one case has been reported thus far [2]. Here, we report a case of bilateral dermoid cysts on the lateral ends of the eyebrows.
A 13-year-old child visited our clinic for an evaluation of masses on both eyebrows (Fig. 1). According to the medical history obtained from his parents, the masses were palpable from birth and had been growing very slowly. The patient was otherwise asymptomatic and did not have any visual compromise. Each mass was cystic and measured approximately 1 cm×1 cm; the two masses appeared symmetrically on the superolateral aspects of the orbital rim. The cysts were soft, movable, and not tender, and there was no evidence of an influence on the other structures. For an exact evaluation of the masses, computed tomography (CT) with enhancement was performed. CT showed bilateral cystic masses on both zygomaticofrontal areas. The left cyst measured approximately 1.1 cm×0.7 cm and the right one, 1.3 cm×0.7 cm. There was no intraorbital or intracranial involvement (Fig. 2). Further, no deformity of bony structures under the masses was observed.

The two masses on both eyebrows existed at birth and had grown since then. Each mass was found to be cystic upon palpation.
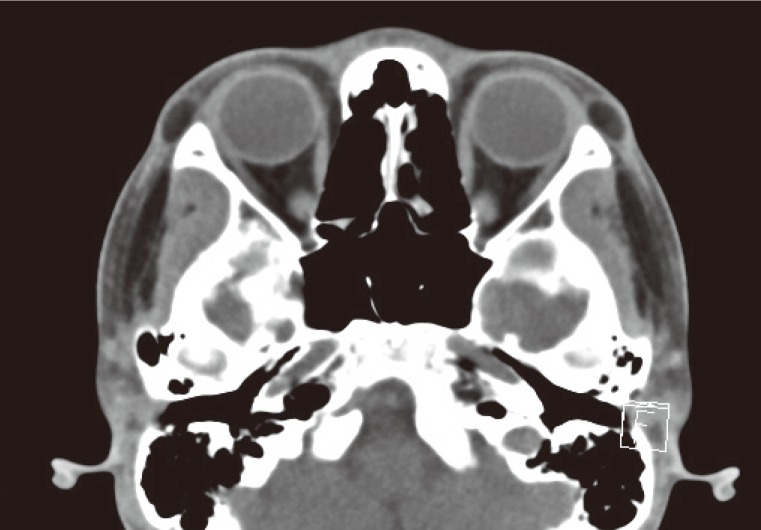
Computed tomography shows bilateral cystic masses on the lateral orbital rims.
We planned the excision of the masses under local anesthesia. Via incision on the inferior margin of the lateral ends of the patient's eyebrows and meticulous subcutaneous dissection, we excised the masses completely without rupture (Fig. 3). There was dense adhesion between the periosteum and the cysts. The right cyst was slightly bigger than the left one, approximately 1.5 cm×0.9 cm vs. 1.2 cm×0.7 cm. After the excision of the masses, shallow imprints of the masses were visible on the underlying bone. The incisions were sutured with 5-0 polydioxanone and 6-0 nylon.

The masses were excised without rupture, and the right mass was slightly larger than the left one.
Pathologic diagnosis confirmed that the two masses were dermoid cysts. There were no complications, and the incisions healed with acceptable scarring and a camouflage effect. The depressed contour deformities recovered after a few months.
Dermoid cysts are benign tumors that can be found throughout the body. These cysts on the face and neck are frequently found in children. New and Erich classified dermoid cysts on the basis of their location. The most frequently involved area is the periorbital area, followed by the nasal dorsum, submental area, and the suprasternal area [1]. Periorbital dermoid cysts are congenital tumors that appear along the naso-optic groove between the maxillary and the mandibular processes during embryonic closure (i.e., the frontonasal and frontozygomatic suture line). Dermoid cysts contain cells of a dermal or an epidermal origin. When a cyst ruptures because of trauma or infection, keratin can cause inflammation and a granulomatous reaction.
Further, periorbital dermoid cysts often have intracranial or intraorbital effects. These effects progress slowly, and when presented later in life, they may cause proptosis, strabismus, globe dystopia, visual field defects, dehiscence of the frontozygomatic suture, and swelling of the temporalis fossa. Such an extension of lateral brow dermoid cysts is a rare but distinct possibility. Therefore, imaging studies such as CT and magnetic resonance imaging are necessary before surgical excision.
The treatment for a periorbital dermoid cyst is surgical excision. There is no consensus on the appropriate timing of the excision. Because dermoid cysts grow with the child and there is a chance of rupture, excision should be performed [2]. In order to decide on the timing of the excision, the size of a dermoid cyst, presence of symptoms, and parents' needs should be considered. Thus far, superficial dermoid cysts on the lateral orbit, as in our case, have been excised through direct incision, upper eyelid crease incision, and an endoscope-assisted approach. If we consider only aesthetics, the endoscopic technique is preferable. However, c onsidering cost effectiveness and hair loss, upper eyelid crease incision is a better approach. To remove a cyst completely and to avoid rupture, a meticulous dissection technique is required as it prevents postoperative complications such as inflammation caused by dermoid components. However, there is always a shallow depression on the bone. Sometimes, this depression is sufficiently large to cause a depressive contour deformity. To prevent such a postoperative depression, Lee and Persing proposed a method of reconstruction using preaponeurotic orbital fat flaps as fillers [3].
Bilateral facial masses are not commonly encountered. If there are symmetrically bilateral masses on someone's face, people may consider them natural and not abnormal and clinicians may also ignore them. Further, the lateral end of an eyebrow has a slight natural protrusion, and bilateral dermoid cysts on the lateral ends of eyebrows may be more prone to misdiagnosis. Therefore, a patient with bilateral masses on his face should be examined carefully, with consideration of a potentially unusual diagnosis.
Notes
No potential conflict of interest relevant to this article was reported.