Congenital Multiple Metatarsal Synostoses with Proximal Phalangeal Deformities of the Foot
Article information
Congenital foot abnormalities such as syndactyly, polydactyly, and brachymetatarsia are commonly seen by plastic surgeons. There have been reports of cases of congenital synostosis of the foot, with the majority of cases involving the rear foot and midfoot (Boccio et al. [1]). However, to the best of our knowledge, multiple metatarsal synostoses with proximal phalangeal deformities is extremely rare and independent from any syndromes and congenital anomaly patterns.
A 28-year-old woman was referred to our plastic surgery outpatient clinic with a chief complaint of pain and deformity in her right forefoot. There were deformities of the right fourth and fifth toes, making it difficult for her to purchase ready-made heeled shoes. The patient had a history of depression, but it was controlled with no adverse effects on her daily life. No other relevant past history or family history was present. A clinical examination demonstrated abducted fourth and fifth toes, and the interdigital side of the first toe and the dorsal sides of the fourth and fifth toes had callosities (Fig. 1). The left foot was normal in all respects.

Preoperative photograph illustrating the fourth and fifth toe deformities of the right foot.
Radiographs showed metatarsal synostoses from the third to the fifth metatarsal bones, and the third metatarsophalangeal joint was comprised of the third and fourth proximal phalanges and the third metatarsal bone (Fig. 2). In this case, dysfunction was not severe, and a minimally invasive operation was planned.

Preoperative radiograph of the right foot showing the synostoses and the third metatarsophalangeal joint malformation.
The operation was performed using an open method. First, the extensor tendons of the fourth toe were kept; then a wedge osteotomy at an angle of 30 degrees was performed, followed by abduction and reduction of the shaft of the fourth proximal phalanx. Finally, the lateral surfaces of the bones were perforated and fixed by crossing soft wire using the two-dimensional intraosseous wiring technique (Moriya et al. [2]). This technique provides stronger fixation between the bones with its tension band function.
Titanium plate fixation was added on the lateral side of the proximal phalanx to ensure more reliable stability. The fifth toe was reshaped to be the same as the fourth toe (Figs. 3, 4). Non-weight-bearing rehabilitation continued for one month after the operation. The foot decreased in width, and pressure on the interdigital side of the first toe was relieved. Consequently, the callosities on the foot disappeared completely.
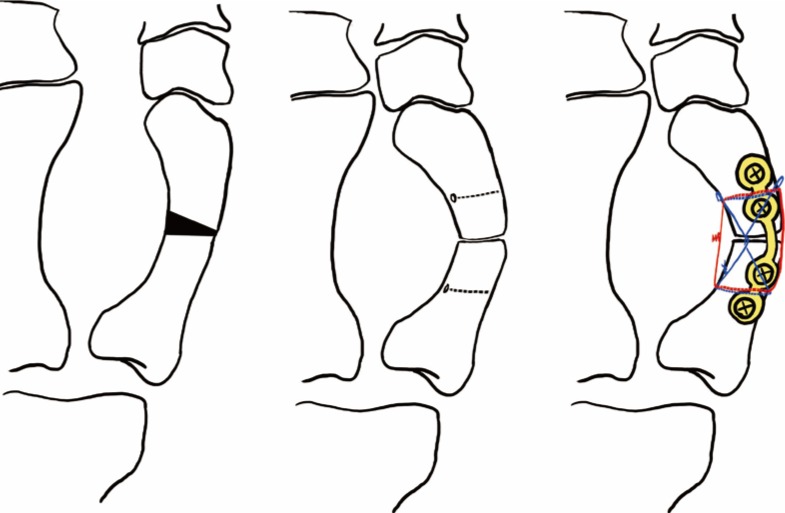
The schema of the osteotomy and the two-dimensional intraosseous wiring technique fixation for the fourth and fifth proximal phalanges.

Postoperative dorsal radiograph.
The patient has good foot alignment that has been maintained for more than one year postoperatively (Fig. 5). The patient can now wear heeled shoes without any pain.

Photograph of the right foot at one year postoperatively.
Metatarsal synostosis occurs as one of the components of some congenital malformation syndromes: Pfeiffer syndrome, Apert syndrome, and Townes-Brocks syndrome. The responsible genes and mode of inheritance have been identified in these syndromes, but isolated cases are rare, and very few cases have been reported; thus, their epidemiology and pathogenesis are unknown. A case of non-syndromic distal metatarsal synostosis of the fourth and fifth toe was described in 2014 (Aspros et al. [3]), but a report of multiple metatarsal synostoses as in this case could not be found.
The hypoplasia of the fourth metatarsal bone and the deformities of the fourth and fifth toes suggest the possibility of a variant of cleft foot with a normal number of toes.
Blauth and Borisch [4] described metatarsal hypoplasty or synostoses in a study on the classification of cleft feet. Partial synostoses usually occurred at the distal parts of the phalanges or metatarsal bones; most frequently, the first and second metatarsals. The third, fourth, and fifth toes were partially or completely synostotic (Blauth and Borisch [4]).
Ogino and Kato [5] described six cases of cleft hand with a normal number of fingers as well. Some anomalies of the adjacent fingers were recognized in several cases, including cutaneous syndactyly, brachymesophalangy, and central polydactyly. They considered the cause of cleft hand without absence of the finger as a failure of separation of the finger rays. This assumption is now accepted as “cleft of the palm”, which is classified as a type of abnormal induction of the digital rays in the modified International Federation of Societies for Surgery of the Hand classification.
Ogino and Kato found another trend, in that the cleft in cases of cleft hand without absence of the finger was not much more severe than with absence of the finger (Ogino and Kato [5]). Given the literature, it is possible that the present case is “mild abnormal induction of digital rays,” though we were not able to find a cleft involving the foot. However, it is very difficult to make a fair judgment on the classification of this case. Further studies of the cause of this congenital foot abnormality are needed.
Notes
No potential conflict of interest relevant to this article was reported.