Transient Exotropia after Open Reduction of a Naso-Ethmoidal-Orbital Fracture
Article information
Exotropia is a form of strabismus in which the eyes turn outward, and can involve various etiologies, durations, and degrees of deviation [1]. Exotropia is caused by the dysfunction of ocular movement resulting from brain damage, nerve injury, or muscle injury. In particular, acquired exotropia is caused by facial trauma, especially blow-out fractures [2]. Generally, cases of acquired exotropia are related to mechanical entrapment of the medial rectus muscle or soft tissue, as confirmed by physical examination and computed tomography (CT). The mechanical entrapment is relieved by surgery [3]. However, some cases are asymptomatic, involving unchecked dysfunction of the ocular muscles caused by a nerve injury and resulting in retraction of the muscle. In this report, we describe a case of transient exotropia after the open reduction of a naso-ethmoidal-orbital fracture without mechanical entrapment.
A 39-year-old male visited the emergency room of our hospital after a motor vehicle accident. A type II bilateral naso-ethmoidal-orbital fracture without medial rectus muscle entrapment (Fig. 1) was diagnosed on a CT scan. On physical examination, diplopia and exotropia were absent, cardinal ocular movement was not limited, and all ocular functions, including intraocular pressure (IOP) and eyesight, were normal.
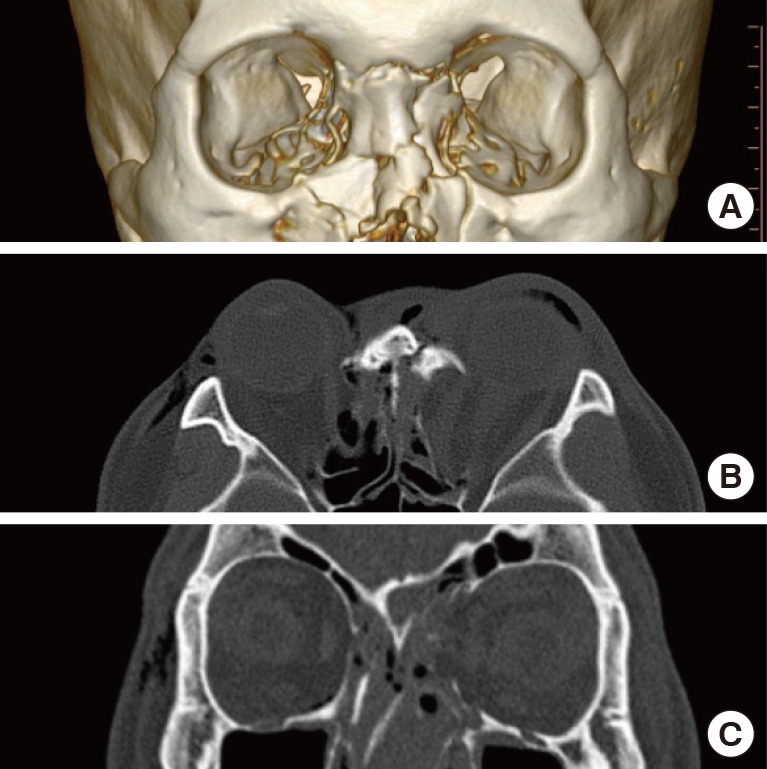
Preoperative computed tomography view of a type II bilateral naso-ethmoidal-orbital fracture. (A) Three-dimensional view. (B) Two-dimensional axial view. (C) Two-dimensional coronal view.
After monitoring the edema around the patient's eyes for eight days, we performed open reduction and internal fixation of the frontal bone via direct incision and orbit wall reconstruction with bio-resorbable co-polymers (Inion, Weston, FL, USA; 1.5-mm mesh) via subciliary skin muscle flap incision were performed under general anesthesia. The intraoperative forced duction test and the medial rectus muscle were normal, with no signs of entrapment.
On the first postoperative day, serious edema and pain during ocular movement appeared in the left eye. In addition, diplopia and limitation of ocular movement were noted (Fig. 2). Every day until the third postoperative day, in conjunction with the department of ophthalmology, the exotropia in the patient's left eye was evaluated, and the IOP, light reflexes, and fundoscopic findings were normal. Hertel's exophthalmometer confirmed and quantified the extent of exophthalmia of the left eye, with protrusion of 13 mm in the right eye and 16 mm in the left eye. Examination of the ocular movement associated with strabismus confirmed 70 prism diopters of exotropia and 25 prism diopters of hypertropia in the left eye. These symptoms lasted until the eighth postoperative day, with non-specific CT findings (Fig. 3). We therefore planned surgical exploration.
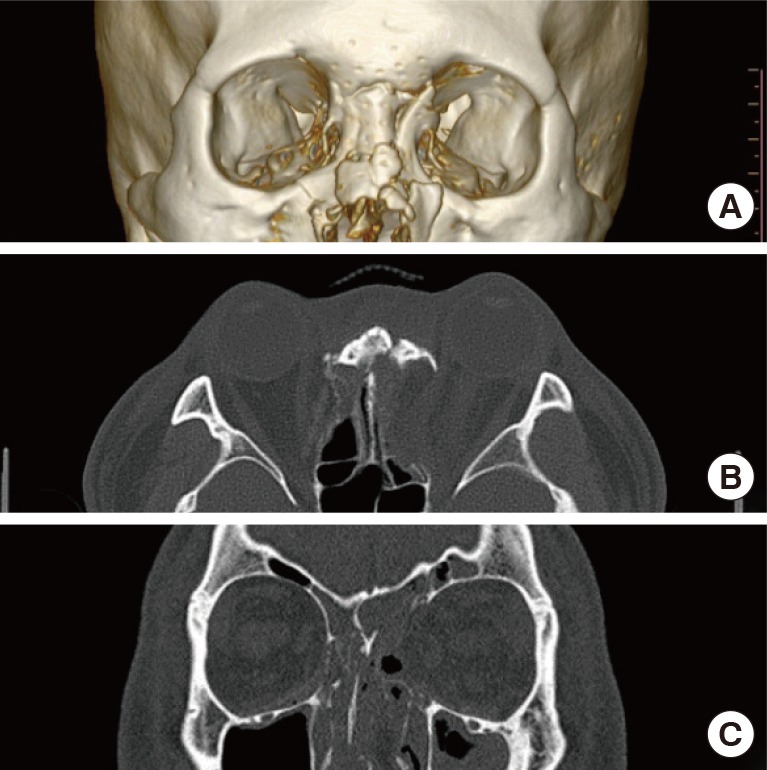
Computed tomography imaging performed on the eighth postoperative day. The inserted plate was non-specific and no muscle entrapment was observed. (A) Three-dimensional view. (B) Two-dimensional axial view. (C) Two-dimensional coronal view.
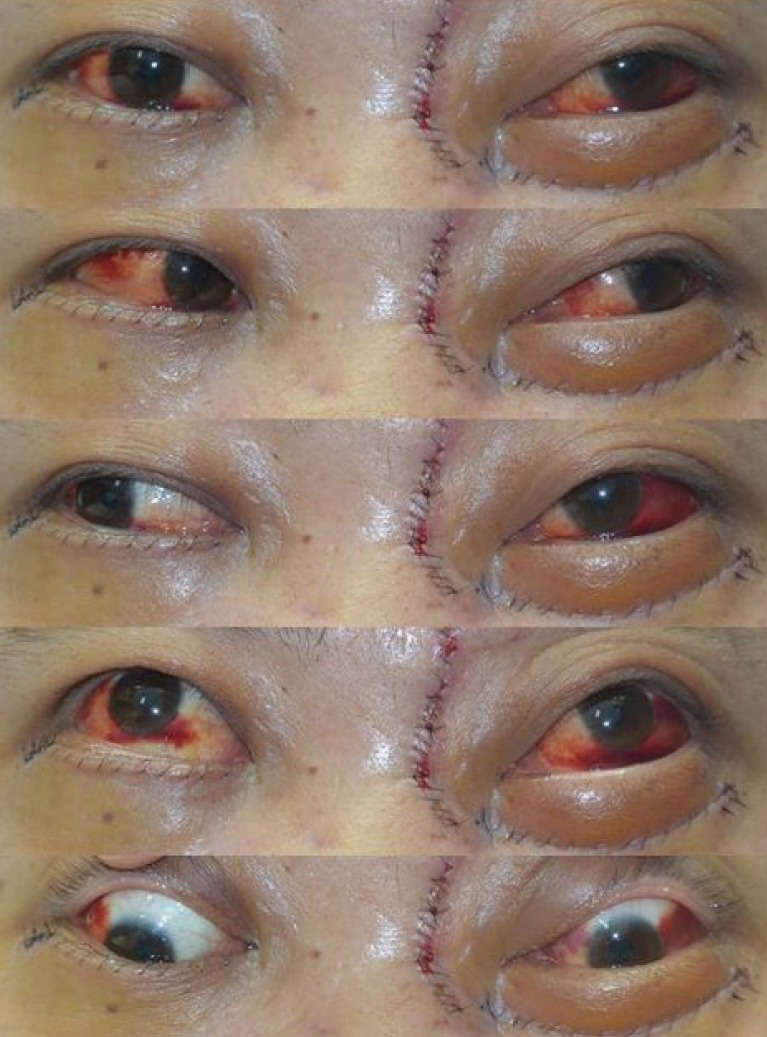
Postoperative day two. The patient complained of diplopia, mild exotropia, and limitation of ocular movement, especially in the downward and medial gazes.
When propofol (Anefol) and rocuronium bromide (Esmeron) were administered for general anesthesia, the normal axis of the left globe in the front-facing gaze appeared to recover, and the forced duction test was in the normal range. Nonetheless, exotropia and limitation of ocular movement in the left eye were still present in an ocular examination performed immediately after the operation (Fig. 4).

Postoperative view two hours after surgical exploration. The left eye symptoms were still present.
Steroid injection therapy (5 mg of dexamethasone, 1 ampule intravenously, three times per day) and a muscle relaxant (Mulex, 1 tablet orally, two times per day) were administered to the patient for five days. No dramatic effect occurred, as when the patient was under general anesthesia, but the exotropia and limitation of ocular movement improved gradually, as well as the patient's discomfort.
The patient was discharged from the hospital seven days after exploration and 15 days after the first operation. The patient's symptoms were evaluated one week, two weeks, one month, and four months after surgery. The patient had normal ocular movement and function, with no complications observed over nine months of monitoring (Fig. 5).

Postoperative view at nine months. The exotropia and limitation of ocular movement in the left eye had completely recovered.
Ocular movement is regulated by the interaction of the four rectus muscles and two oblique muscles that act jointly or separately, depending on whether the nerves innervating the muscles are intact and functioning. Damage to one or more of these muscles or nerves leads to a disruption of the interaction among the ocular muscles, which may cause symptoms such as diplopia or limitation of ocular movement [4]. Mechanical entrapment of the medial rectus muscle or the soft tissue is the most common cause of exotropia. In our case, mechanical entrapment was absent and the exotropia improved briefly in response to a muscle relaxing agent (Esmeron) alone, without the application of external force. The Mulex used postsurgically had no additional effect, but the patient's symptoms then resolved spontaneously.
Intraoperatively, none of the ocular muscles were found to be trapped and the implant was located in the correct position. It is likely that our patient suffered from dysfunction of the medial rectus and superior oblique muscles due to intraoperative retraction and the resulting external force generated by the eyeball. The exotropia was possibly caused by an imbalance in muscle tonus that led to the appearance of normal function of the superior and lateral rectus muscle when the medial rectus and superior oblique muscle had functionally deteriorated.
We experienced a case of transient exotropia with spontaneous recovery after the open reduction of a naso-ethmoidal-orbital fracture without mechanical entrapment.
Notes
No potential conflict of interest relevant to this article was reported.