The Surgical Impact of E-Cigarettes: A Case Report and Review of the Current Literature
Article information
Abstract
We report a case of a 51 years old female with a 25 pack year smoking history who underwent bilateral mastectomy and immediate tissue expander reconstruction for newly diagnosed right breast cancer. The patient reported herself as a non-smoker despite significant e-cigarette use, with resulting significant mastectomy skin flap necrosis and breast reconstruction failure. Little is known about the physiologic effect of e-cigarettes on wound healing and tissue perfusion. To this end, we provide an updated review of the impact of e-cigarettes on surgical outcomes. PubMed, Ovid MEDLINE, and PRS GO were searched for the terms “e-cigarette”, “electronic cigarette”, “e-cig”, “electronic nicotine delivery system”, “vaping”, “surgery”, “surgical”, “peri-operative”, “operate”, “operative”, and “wound healing”. Abstract review of all articles was performed. 123 articles returned that contained both variants of e-cigarettes and surgery as keywords. Of those, manual assessment returned three articles which were found to be relevant to e-cigarette use in the surgical patient. No articles were found that compared perioperative complications in e-cigarette versus traditional cigarette users in humans. In conclusion, our case report depicts the potential dangers associated with e-cigarette use in the surgical patient. There is a public misconception that e-cigarettes are healthier than traditional cigarettes and as such their use may go unreported by patients. Early evidence suggests e-cigarettes may induce some of the same physiologic changes as traditional cigarettes, and may have a significant deleterious effect on wound healing.
INTRODUCTION
Electronic cigarettes (e-cigarettes) are rapidly gaining popularity as a nicotine alternative to traditional cigarettes. Common reasons for using e-cigarettes include the perception they are healthier than traditional cigarettes and to aid in smoking cessation [1]. Despite increasing usage, there is a paucity of data on the physiologic impact of this nicotine supplement on surgical outcomes. We present a case of significant skin flap necrosis and breast reconstruction failure following bilateral mastectomy and immediate tissue expander reconstruction after a patient reported to be a non-smoker despite significant e-cigarette use. We further provide a review of the literature concerning the impact of e-cigarettes on surgical outcomes.
METHODS
Pubmed and Ovid MEDLINE were queried for the terms “e-cigarette”, “electronic cigarette”, “e-cig”, “electronic nicotine delivery system”, “vaping”, “surgery”, “surgical”, “peri-operative”, “operate”, “operative”, and “wound healing”. Eligible articles included animal studies, clinical trials and reviews of the literature (including opinion pieces) if they pertained to e-cigarette use in the perioperative period. Search was limited to publications in the English language through June of 2016. Data extraction included patient willingness to try e-cigarettes for smoking cessation in the perioperative period, effects on postoperative complications and surgeon opinion on e-cigarette use in the perioperative period.
RESULTS
The literature search returned 123 articles, which underwent title review. Of those, 29 underwent manual full text review, from which three articles were found to be relevant to e-cigarette’s impact on surgical outcomes.
While an abundance of opinion pieces and summaries of e-cigarette use and potential hazards exist, only these three articles commented on possible complications associated with e-cigarette use in surgical patients. One was a published abstract by Rau et al. [2], which studied the effect of tobacco cigarette smoke, 1.2% e-cigarette vapor and 2.4% e-cigarette vapor on random pattern flaps compared to room air in rats. It was found that all three study groups were not significantly different from each other and all experienced a significantly higher percentage of flap necrosis than the rats exposed to room air. The second was a pilot study showing study subjects smoking electronic cigarettes exhibited decreases in cutaneous blood flow [3]. The third was a case report by Krishnan et al. [4] which reported a case of bilateral muscle-sparing transverse rectus abdominis (TRAM) flaps that experienced multiple episodes of vasospasm in a woman smoking e-cigarettes. Upon operative exploration the arterial and venous anastomoses were noted to be intact without kinking and the patient was started on oral Nifedipine daily for presumed vasospasm with subsequent uneventful postoperative course. Summaries of these three articles can be found in Table 1.
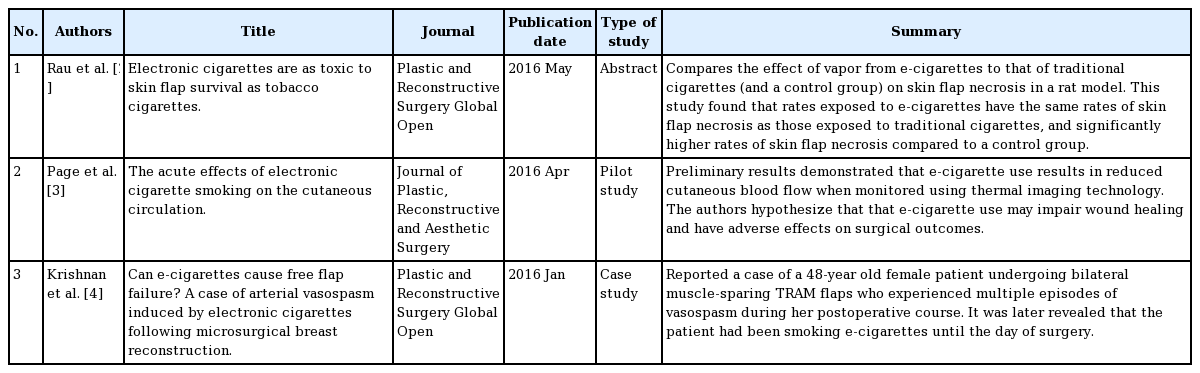
Articles related to the effect of e-cigarettes on surgical outcomes
Case
A 51-year-old female with a 25 pack year smoking history and newly diagnosed right breast cancer underwent right skin sparing mastectomy with sentinel lymph node biopsy, left prophylactic skin sparing mastectomy and immediate tissue expander reconstruction at our institution. The patient had right breast stage IA multifocal invasive ductal carcinoma and multifocal ductal carcinoma in situ (DCIS). Margins were negative with invasive carcinoma closest at 0.7 cm and DCIS closest at 0.5 cm. Sentinel lymph node biopsy was negative for metastatic carcinoma. The patient denied history of coronary artery disease, myocardial infarction, congestive heart failure, diabetes mellitus, kidney or lung disease, venous thromboembolism, or any bleeding disorders. She likewise denied drug use or daily alcohol consumption. Having stopped smoking for several months prior to the surgery, the patient did not consider herself a smoker and reported herself as a “non-smoker”. On physical examination, she had 40 DD cup breasts with grade 3 ptosis. The patient was deemed an American Society of Anesthesiologists Physical Status of 2, indicating mild systemic disease. She was a good candidate for skin sparing mastectomy because her breasts were not pendulous. 700 mL fill tissue expanders were placed sub-pectorally with Flex HD support for the inferolateral breast pocket. Each expander was filled with 500 mL intraoperatively. At conclusion of the mastectomy, her flap appeared viable with good capillary refill. At completion of expander placement, her flaps continued to appear very viable. Her postoperative course was complicated by extensive bilateral mastectomy skin flap necrosis (Fig. 1). This was managed with tissue expander removal, debridement and primary closure two weeks after her initial surgery given the need to start chemotherapy. It was only after post-hoc questioning that the patient revealed that she was actively engaging in e-cigarette use. Indeed, she noted switching to e-cigarettes approximately 3 months prior to her surgery due to the belief they were safer than traditional cigarettes and maintained a usage similar to her previous 1.5 pack per day amount.

Mastectomy skin flap necrosis in patient using e-cigarettes
A 51-year-old female with a 25 pack year smoking history underwent bilateral mastectomy and immediate tissue expander reconstruction for newly diagnosed right breast cancer at our institution. Her postoperative course was complicated by extensive bilateral mastectomy skin flap necrosis, as demonstrated here. This photograph was taken approximately 3 weeks after mastectomy and tissue expander insertion.
DISCUSSION
It is well-established smoking in the perioperative period negatively impacts surgical outcomes. Specific to plastic surgery procedures, nicotine mainly increases risk of skin flap necrosis and surgical site infection [5]. Smokers undergoing facelifts have a 13-fold increased risk of skin flap necrosis compared to non-smokers [6]. Smokers undergoing TRAM breast reconstruction have higher rates of mastectomy and abdominal skin flap necrosis, with rates markedly increased after a 10 pack year smoking history [7]. Patients undergoing head and neck reconstruction have significantly higher wound complications with preoperative cotinine levels above 10 mg/dL, giving a measurable target for when smoking interventions could be beneficial to outcomes [8]. Controversial findings exist with regard to cigarette smoking’s effect on free flap outcomes; some suggest smoking decreases rates of microvascular anastomosis patency with resulting increases in flap loss while others find no effect [7,9,10]. A thorough summary of the negative effects of smoking on a whole range of plastic surgery procedures was described by Rinker [11] in 2012.
With increasing awareness of the adverse effects of traditional cigarette smoking, alternative nicotine options are gaining popularity. E-cigarettes are one such option. Marketed as “healthier” and “cleaner”, they are often viewed as a better option to traditional cigarettes [12].
While traditional cigarettes deliver a host of toxic agents in addition to nicotine, the content of e-cigarettes is less well known (Table 2). Nicotine delivery may actually be similar to that of traditional cigarettes, though there is inconsistency between labeled and actual nicotine content of e-cartridges, as well as between nicotine levels in cartridges versus the aerosolized form [13]. Inconsistencies are also seen in plasma nicotine levels; while levels seem to be lower in those using nicotine replacement therapy compared to traditional cigarettes, similar rises are seen after smoking e-cigarettes and traditional cigarettes [14,15]. Ultimately, nicotine levels are largely dependent on patient smoking habits, which can vary widely.
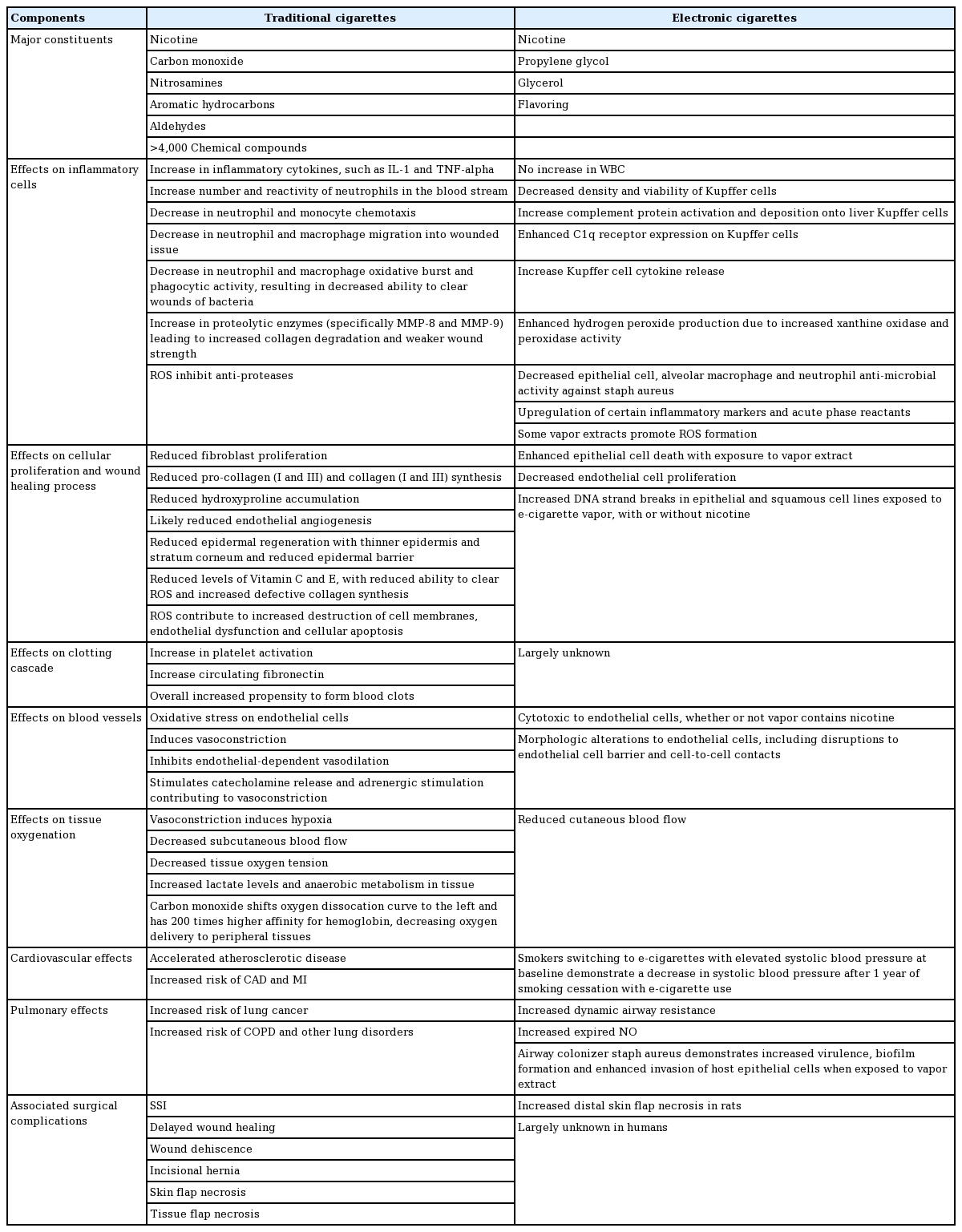
Comparison between traditional cigarettes and e-cigarettes
E-cigarette vapor also demonstrated cytotoxicity to endothelial cells, whether or not nicotine was present. Additionally, despite Groniewicz findings of decreased nitrosamines in the 11 e-cigarette brands tested, there still remains significant variability among brands [16]. In fact, e-cigarettes can contain more nicotine than traditional cigarettes. E-cigarettes may have just as much of a detrimental effect on tissue oxygenation as traditional cigarettes given study subjects demonstrated decreases in subcutaneous blood flow with e-cigarette use [3].
Marketing of e-cigarettes relies heavily on the perception that they have a role in smoking cessation programs. Unfortunately, several studies have shown e-cigarette users have lower rates of smoking cessation compared to never users [12,17]. Other studies have shown e-cigarettes may aid in smoking cessation with quit rates similar to that of other nicotine replacement strategies and may have a more beneficial effect in reducing the number of cigarettes consumed per day [18]. However, without more data on complication rates of e-cigarettes in surgical patients, using them to assist with smoking cessation prior to surgery is of unknown benefit. Given that many smokers undergoing elective surgery have expressed interest in using e-cigarettes as a means to abstain from smoking in the perioperative period, more data about their safety must be evaluated [19]. Despite limited objective data, evidence suggests e-cigarettes may induce some of the same physiologic changes as traditional cigarettes, with or without nicotine present, and may have a significant deleterious effect on wound healing.
Limitations
Our review of the literature demonstrates the lack of data published about e-cigarettes in a surgical population and some suggestion of association with complications such as skin necrosis and vasospasm. As such, they should be considered equivalent to traditional cigarettes until more information about their safety and toxicity is available, particularly in plastic surgery patients undergoing elective operations. This review is limited by a focus on the surgical literature and did not delve into general reviews of e-cigarettes in the medical literature. It is also significantly limited by the paucity of available objective data on e-cigarettes in the surgical literature, as can be seen from the lack of randomized, controlled trials.
Notes
No potential conflict of interest relevant to this article was reported.
Notes
PATIENT CONSENT
The patient provided written informed consent for the publication and the use of their images.