Retiform Hemangioendothelioma on the Finger
Article information
Retiform hemangioendothelioma was differentiated from low-grade cutaneous angiosarcoma by Calonje et al. [1] in 1994; retiform hemangioendothelioma is a very rare tumor of the blood vessels, with less than 30 cases reported throughout the world [2]. The causes of retiform hemangioendothelioma are unknown [2]. Clinically, this tumor occurs mainly in the limbs of young adults, with greater occurrence in the lower limbs, but occasional cases in the trunk, head, and penis [1,3]. Although metastasis or malignancy is rare, retiform hemangioendothelioma is known to recur in approximately 50% of cases [3].
No cases of retiform hemangioendothelioma have previously been reported in Korea. The authors describe the case of a Korean patient diagnosed with retiform hemangioendothelioma.
A 20-year-old male patient without any medical history of interest visited the department of plastic and reconstructive surgery of Dankook University Hospital with a mass on the middle phalanx of the left index finger (Fig. 1). The mass began to form about 6 years ago and was gradually enlarged; the patient did not have any history of a wound or a mass in the same region. A soft and compressible protruding mass, with a dimension of 1.5×1×1 cm, was observed. Although there was no open wound, the patient complained of pain when pressed. The finger distal to the mass had normal circulation and sensation. Angiography carried out prior to surgery revealed that the mass corresponded to an angioma (Fig. 2).

Clinical photograph of retiform hemangioendothelioma on left index finger.
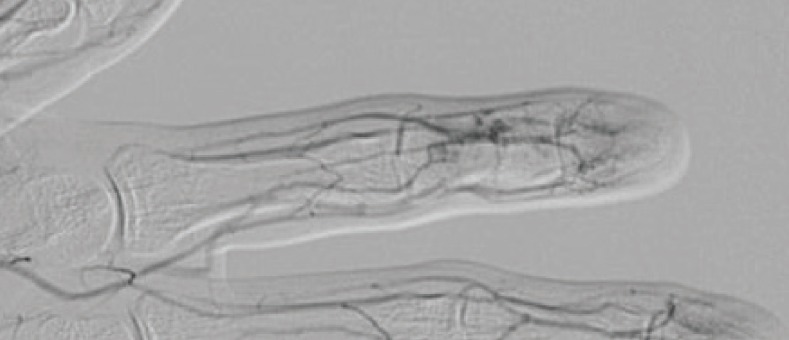
Arteriography showing increased focal vascularity on the left index finger during the capillary phase.
The patient was administered general anesthesia since the mass was located below the dermis and its boundary was not clear; skin was incised vertically over the mass and 3 mm of normal surrounding soft tissue was excised with the mass. During the excision, the mass did not present any signs of infection or inflammation. Following the excision, the size of the mass was 0.5×0.4 cm, which was considerably smaller than the size prior to excision.
Histologically, the lesion was not well demarcated and was composed of elongated and branching blood vessels arranged in a retiform pattern (Fig. 3). The blood vessels were lined with hobnail endothelial cells with focal papillary projections. The endothelial cells revealed enlarged nuclei with vesicular chromatin and rare mitosis. Some lymphocytic infiltrate was observed. Immunohistochemically, the endothelial cells were diffusely positive for factor VIII-related antigen (Fig. 4).
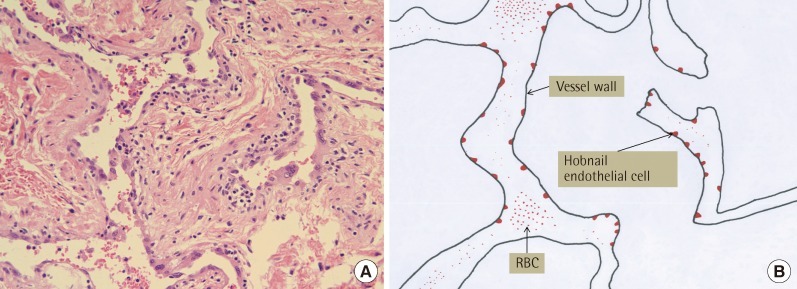
(A) Microscopic findings of retiform hemangioendothelioma (H&E, ×200). (B) Diagrammatic representation of the branching blood vessels lined with hobnail endothelial cells with focal papillary projections. RBC, red blood cell.
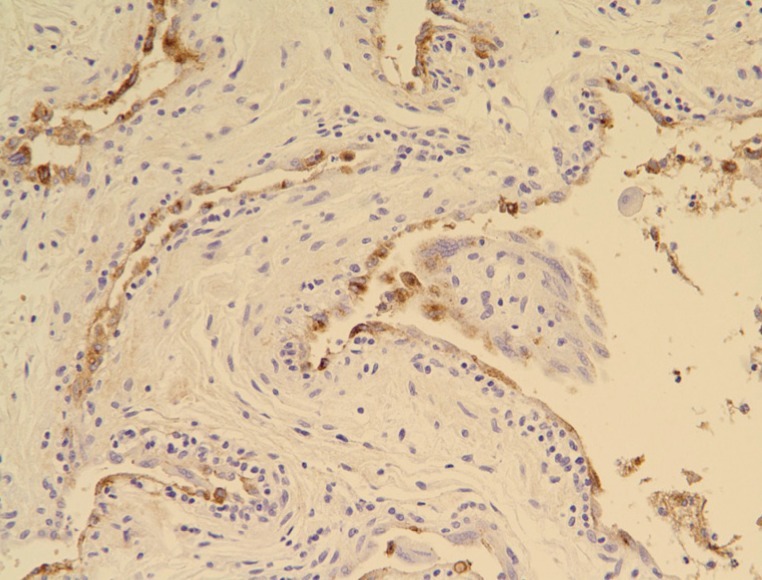
Microscopic findings of retiform hemangioendothelioma. Endothelial cells were immunoreactive to factor VIII-related antigen (Immunohistochemistry, ×200).
The patient was diagnosed with retiform hemangioendothelioma and recovered without complications. However, 2 months after surgery, the tumor had recurred, and the patient was lost to follow-up. Retiform hemangioendothelioma was first considered to be a disease entity separate from low-grade cutaneous angiosarcoma in 1994 [1]. Cutaneous angiosarcoma has a dismal prognosis, with a high incidence of recurrence and metastasis and a high mortality rate [1]. Retiform hemangioendothelioma also has a high local recurrence rate; however, this tumor rarely metastasizes, and no tumor-related deaths have been reported to date [2,3].
Although retiform hemangioendothelioma occurs across a diverse age range, it is most common in young or middle-aged adults, with a greater frequency in females [1,3]. It mostly occurs in the limbs, with a higher incidence in the lower limbs [1,3]. But in the trunk, head, and penis, cases occasionally occur [1,3]. Retiform hemangioendothelioma mostly occurs as an asymptomatic, slow-growing single lesion [3]. However multiple, rapid-growing cases have been reported [3,4]. The duration of lesion varies between 2 months to several years [3]. Most cases are presented as exophytic, dermal, or subcutaneous nodules or plaques with a size range of 1 to 30 cm [3].
The etiology of retiform hemangioendothelioma remains unknown. However several reports have proposed its association with human herpesvirus-8, lymphedema, previous radiation treatment, and non-epidermal malignant tumors [1,2].
Local recurrence is observed in almost half of all cases of retiform hemangioendothelioma [3]. A single case of localized lymph node metastasis and one case of soft tissue metastasis have been described, but there have been no reports of remote metastasis or death clearly related to the mass [2,3]. As there is no characteristic clinical symptom helpful in diagnosing retiform hemangioendothelioma, biopsy is the only diagnostic method available at present [1,3,5]. The differential diagnosis of retiform hemangioendothelioma includes Dabska's tumor, malignant lymphoma, dermatofibrosarcoma protuberans, bacillary angiomatosis, Kaposi's sarcoma, targetoid hemosiderotic hemangioma, and cutaneous angiosarcoma [1-3]. Histologically, retiform hemangioendothelioma is characterized by long arborizing vascular channels lined with hobnail endothelial cells. The vascular channels are arranged in a retiform pattern, which mimics normal rete testis. Prominent stromal lymphocytic infiltrates are often observed. Immunohistochemically, the endothelial cells express endothelial markers such as CD31, CD34, factor VIII, and Ulex europaeus agglutinin-1 [1].
Due to its high incidence of local recurrence, the treatment of choice for retiform hemangioendothelioma is a wide surgical excision with histopathologically tumor-free margins and long-term follow-up is essential. In cases with lymph node metastasis, radiation therapy has been reported to be successful [1]. In addition, in unresectable retiform hemangioendothelioma was successfully treated with low-dose cisplatin and moderate radiotherapy in one case [2]. In summary, retiform hemangioendothelioma is a rare vascular neoplasm of low malignant potential with a high recurrence rate, most often occurring on the extremities of young adults. To our knowledge, this is the first case of retiform hemangioendothelioma reported in Korea.
Notes
This article was presented at the meeting 68th Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 4-7, 2010 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.