Desmoplastic Fibroblastoma of the Finger Tip in an Adult
Article information
Desmoplastic fibroblastoma is a rare neoplasm characterized by spindle- to satellite-shaped fibroblastic cells that are sparsely distributed in a collagenous stroma. It was first described in 1995 by Evans [1], who reported seven cases of morphologically distinct, benign, fibrous, soft tissue tumors and gave this specific tumor type its name.
Since the characterization of this tumor by Evans, fewer than 100 cases have been reported in the English literature. Only 7.9% of 63 cases of desmoplastic fibroblastoma in one analysis were hand lesions. Furthermore, there is only one report of a finger lesion, which developed in the volar aspect of the metacarpophalangeal joint of the left little finger [2].
Clinically, desmoplastic fibroblastoma manifests as a painless, slow-growing mass of more than six months duration. It usually appears between the ages 25 to 83 years in the neck, forearm, shoulder, thigh, or feet. Most have been treated by surgical excision and neither local recurrence nor metastasis has been reported [3]. This paper presents a rare case of desmoplastic fibroblastoma of a finger with the clinicopathologic and immunehistochemical findings.
A 65-year-old male visited this clinic for the evaluation of a mass with hard swelling on his right index finger distal phalanx volar area. The mass had been growing slowly for 10 years. On physical examination, a 1.0 cm, well circumscribed, firm, nodular and non-tender mass was palpated (Fig. 1). There was no other specific medical history and the patient was otherwise in good health. A skin sonogram demonstrated a well-defined slightly hypoechoic mass located distal to the insertion site of the flexor digitorum profundus tendon (Fig. 2).
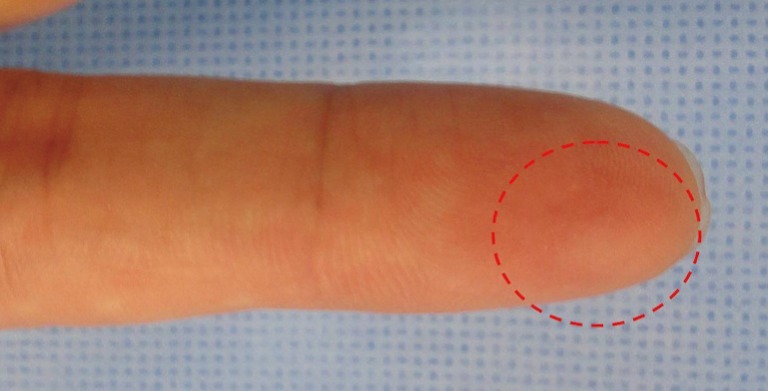
A nodular mass on the distal phalanx of the right index finger. About 1.0 cm sized, a well-circumscribed, firm, nodular and non-tender mass (red dot circle) of about 1.0 cm was palpated.
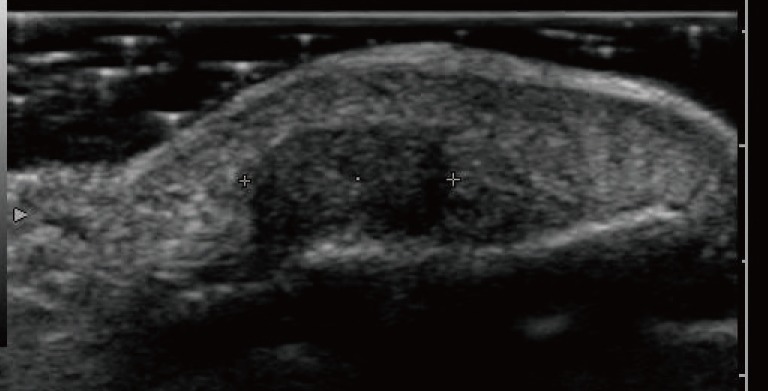
In a skin sonogram, a well-defined, slightly hypoechoic mass was observed distal to the insertion site of the flexor digitorum profundus tendon.
The mass was totally removed by surgical excision. Gross examination revealed a well-demarcated, oval-shaped, fibroelastic mass, measuring 1.0×1.0×0.4 cm. Microscopically, the lesion was well delineated and paucicellular with a prominent collagenous background. The tumor cells had a spindle to stellate shape with thin elongated nuclei. No mitotic figures, calcification, cystic degeneration, infiltration of adipose tissue, or necrosis was found (Fig. 3). Special stains with Masson's trichrome and smooth muscle actin (SMA) were performed (Fig. 4). The collagenous nature of the stroma was confirmed using Masson's trichrome stain and the tumor cells were partially positive with alpha SMA staining. The final diagnosis was desmoplastic fibroblastoma. There was no clinical sign of recurrence for 6 months after excision.
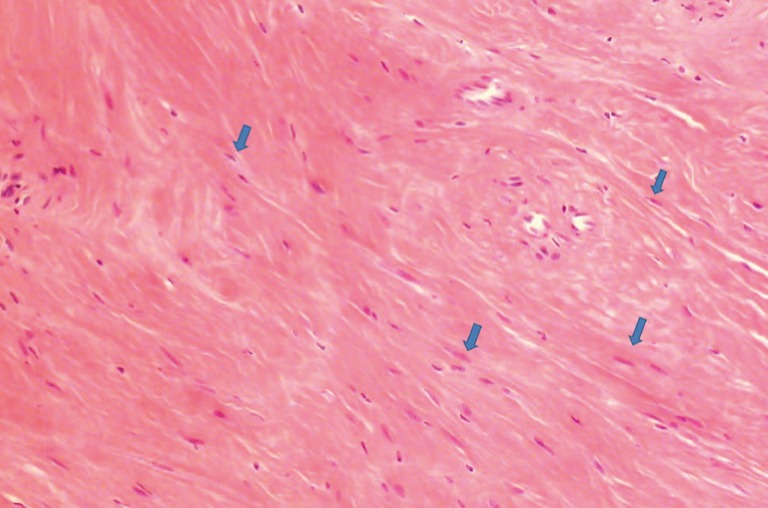
Collagenous fibroma showing scattered stellate-shaped and spindled fibroblasts (blue arrows) in a collagenous background (H&E, ×100).

(A) The collagenous nature of the stroma was confirmed through Masson's trichrome staining (×40). (B) Tumor cells were partially positive for alpha smooth muscle actin staining (×40).
Desmoplastic fibroblastoma typically displays as a painless, mobile, firm and well-circumscribed subcutaneous mass that grows slowly with a duration of enlargement of more than 6 months. The tumors have ranged from 1 to 13.8 cm in size, with a mean size of 4.9 cm. There is no evidence of bone involvement except for a rare case with surface erosion [3].
Immunohistochemical stains are useful in diagnosis, which shows positivity for vimentin and variable expression for alpha smooth muscle actin. The lesion is usually negative for desmin, epithelial membrane antigen, S100, and CD34. A cytogenetically abnormal clone involving the 11q12 breakpoint has been detected in several cases [4]. In our case, immunohistochemical staining for vimentin was not performed. Positivity for vimentin implies that the tumor cells are of fibroblastic lineage. However, we were able to determine that with the satellite to spindle shape of cells.
Histopathologically, the tumors appear well-marginated under low-power microscopic examination. The tumor cells are relatively stellate- and spindle-shaped fibroblastic cells separated by a densely fibrous to fibromyxoid matrix. These fibroblasts lack any atypical or hyperchromatic nuclei. Mitotic figures are very rare or absent, and tumor necrosis is not seen.
A wide variety of benign fibroblastic soft tissue tumors have been classified as fibroma. Among the entities included in this category are the nuchal fibroma, fibroma of the tendon sheath, sclerotic fibroma of the skin, and calcifying aponeurotic fibroma. Evens recently proposed an additional group--desmoplastic fibroblastoma. A general lack of awareness of this poorly recognized entity may lead to misdiagnosis of other soft tissue neoplasms because of the small number of reported examples. Miettinen and Fetsch [5] analyzed sixty-three cases of desmoplastic fibroblastoma from the files of the Armed Forces Institute of Pathology. Fifty-two of these cases were originally diagnosed as other tumors, including fibromatosis (n=18), fibroma (n=15), neurofibroma (n=8), nodular fasciitis (n=3), fibroma of the tendon sheath (n=3), myxoma (n=2) as well as chondroma, myofibroma, and myxoid lipoma (one case of each). The differential diagnosis of desmoplastic fibroblastoma includes benign, locally aggressive, and low grade malignant soft tissue tumors consisting of relatively uniform stellate- or spindle-shaped cells embedded in a myxocollagenous matrix, such as nodular fasciitis, fibromatosis, fibroma of the tendon sheath, nuchal fibroma, sclerotic fibroma of the skin, neurofibroma, solitary fibrous tumor, and low grade fibromyxoid sarcoma. Although desmoplastic fibroblastoma of the finger can be confused with fibroma of the tendon sheath, the latter is deeply attached to the tendon or tendon sheath. From a histological perspective, fibroma of the tendon sheath is more cellular and less homogeneous. It also differs from desmoplastic fibroblastoma because of a lobular growth pattern, with the lobules separated by cleftlike vascular spaces [3,5].
In conclusion, we present a rare case of desmoplastic fibroblastoma that developed on the finger with clinicopathologic and immunohistomchemical features. Typically, this type of tumor has developed as a firm, non-tender, slow growing mass in older males. Complete excision with functional preservation was performed and recurrence was not observed for 6 months after the operation. Despite a very small number of reported cases, desmoplastic fibroblastoma should be considered in a differential diagnosis for soft tissue tumors of the finger.
Notes
This article was presented as a poster at the 69th Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 11-13, 2011 in Seoul, Korea.
This research was supported by Seoul St. Mary's Clinical Medicine Research Program year of 2009 through the Catholic University of Korea.