Establishing cleft services in developing countries: Complications of cleft lip and palate surgery in rural areas of Indonesia
Article information

Abstract
Background
Cleft treatment is frequently performed in Indonesia, mostly in charity missions, but without a postoperative protocol it is difficult to establish the risks and complications of cleft treatment. The present study was designed to give an overview of current cleft lip and palate treatment strategies in Indonesia and to assess the complication rates during and after surgery.
Methods
This prospective study evaluated anesthetic, intraoperative surgical, and short-term postoperative complications in patients undergoing primary, secondary, or corrective surgery for cleft lip and palate deformities. The population consisted of 98 non-syndromic cleft patients. The main anesthetic complication that occurred during general anesthesia was high blood pressure, whereas the main intraoperative surgical complication was excessive bleeding and the main early postoperative complication was extremely poor wound hygiene.
Results
In this study, there were no cases of perioperative or postoperative mortality. However, in 23 (23.4%) of the 98 operations performed, at least one perioperative complication related to anesthesia occurred. The intraoperative and early postoperative complications following cleft lip and/or palate were assessed. There was a significant difference in the complication rate between procedure types (χ2=0.02; P<0.05). However, no relationship was found between perioperative complications related to anesthesia and the occurrence of postoperative complications (χ2=1.00; P>0.05). Nonetheless, a significant difference was found between procedure types regarding perioperative complications and the occurrence of postoperative complications (χ2=0.031; P<0.05).
Conclusions
Further evaluation of these outcomes would help direct patient management toward decreasing the complication rate.
INTRODUCTION
Cleft palate occurs when the palatal shelves fail to close and fuse between weeks 8 and 12 of embryonic development [1]. Some published studies found a significant relationship between socioeconomic status and the diagnosis of non-syndromic orofacial cleft [2,3]. Since Indonesia, as a developing country, has a large poor population, and there are huge financial and educational differences between the higher and lower social classes, those findings are highly interesting in the Indonesian context.
In Indonesian rural areas, charity missions are the only platform through which to offer cleft surgery on a larger scale. A consequence of infrastructural issues in Indonesia is that the country does not offer facial cleft treatment on a nationwide scale, and that insurance companies are only available for the higher social classes and richer population. The Lancet Commission on Global Surgery (2015) revealed that the predicament of untreated surgical conditions was mostly found among individuals living in Low-to-Middle-Income Countries (LMICs). Among LMICs, the lowest income is found among residents of rural areas, and marginalized populations fare the worst [4].
As with other surgical procedures, cleft surgery has inherent risks that can be serious and in the worst cases can be life-threatening [5]. In rural areas of developing nations, including Indonesia, orofacial cleft is associated with elevated infant mortality and significant morbidity [6]. The measurement and evaluation of complications in cleft lip or palate patients, especially those in rural areas, are a challenge for medical professionals. However, no studies have yet provided data on the outcome of techniques used, as well as treatment histories and follow-up data, to provide support for the choices of the Indonesian cleft surgery team.
The purpose of this report was to assess the intraoperative and postoperative complications experienced while providing surgery at charity missions in rural areas of Indonesia. Furthermore, the current cleft rehabilitation strategies and protocols in Indonesia were evaluated, without regard either to the relative merits of particular techniques, or to the results of individual oromaxillofacial surgeons.
METHODS
This is a prospective study that evaluated records from approximately 150 patients who were surgically treated for cleft lip and/or palate between April 1 and June 30, 2014 (all ages included) (Fig. 1). Patients who were treated under local anesthesia and had cleft lip and/or palate induced by trauma or infection were excluded. The study was conducted in accordance with the Declaration of Helsinki.
Subject with complete cleft palate
After obtaining ethical approval from the Health Research Ethics Committee of the Faculty of Medicine, Hasanuddin University, Makassar, Indonesia, surgery was performed (approval number: UH14060319). Prior to surgery, the subjects provided written informed consent for the procedure and data collection. Surgery was done by a team of two oral and maxillofacial surgeons (MR and AT), two doctors in anesthesiology (SKA and AHT), one anesthesia assistant (Adanas Sini), and one dentist general practitioner (ASHY). The procedures were conducted in several private hospitals or care centers and on charity surgery trips: twice in the Toraja district in South Celebes, once in the city of Sidenreng Rappang, and once in Berau, situated on Kalimantan Island (Borneo).
For incomplete cleft palate, both hard and soft, the two-flap technique (Von Langenbeck) was most commonly used, and for bilateral complete cleft palate, a modification of the Veau-Kilner technique (also known as the two-flap-pushback) was used in this study, following common practice in Indonesia (Fig. 2). The surgeon’s choice of a certain technique was mostly dependent on training and exposure to the various techniques available.
Modification of the Veau-Kilner technique
Before further patient data were obtained, a classification of the cleft location and cleft type was performed using the LAHSAL system. After diagnosis and classification, patient data were obtained during the preoperative consultation, about 24 hours before surgery. Even though there were no standardized postoperative instruction forms or protocols, patients and/or their caretakers were well-informed about the wound care instructions and the rehabilitation process.
Cleft lips were treated by a slightly modified rotation advancement method. Isolated cleft palate defects were repaired by the Von Langenbeck and Veau-Kilner techniques. Combined cleft lip and palate defects were treated in a 2-stage repair involving both the Millard rotation advancement technique and the Von Langenbeck technique.
During surgery, surgical complications were assessed. The intraoperative complications were evaluated and divided into two types: complications related to general anesthesia and surgery-related complications. The form used to gather information on complications was a checklist created exclusively for the present study.
When hospitalized after cleft surgery, patients were seen every day and routinely placed on antibiotics by their hospital nurse or doctor (Fig. 3). Any type of postoperative complication was noted in the patient’s handwritten medical chart. All observations during surgery and at postoperative check-up appointments were performed by researchers with extensive experience in the medical field.
Clinical view of the subject after surgery
The statistical analysis was performed using SPSS for Mac version 22 (IBM Corp., Armonk, NY, USA). Continuous and categorical variables were presented as counts and percentages. The Pearson chi-square test was used to analyze the relationship between early postoperative complications and age. The McNemar test was used to compare the complication rates during and after surgery. P-values <0.05 were considered to indicate statistical significance.
RESULTS
This study included 98 of the 112 patients who received cleft surgery (55 males and 43 females), including 31 patients who underwent palatoplasty, 66 who underwent labioplasty, and one who underwent gnathoplasty. Eleven patients who underwent surgery under local anesthesia had to be excluded from the results. Two patients were also excluded because they were diagnosed with macrostomia and one patient was excluded because her cleft was caused by a noma infection.
The overall distribution of age, sex, and treatment types can be seen in Table 1. Patients’ mean age (standard deviation) at the time of operation was 6.5 (7.0) years. Twenty-three patients presented during infancy (≤1 year) and 66 patients presented during childhood (2–17 years). Seven patients (7%) received primary cleft surgery in adulthood. Because of incomplete data on date of birth or age, two patients were excluded from this analysis.

Distribution of age groups, sex, and treatment types
In this study, there were no cases of perioperative or postoperative mortality. However, in 23 (23.4%) of the 98 surgical procedures performed, at least one perioperative complication involving anesthesia occurred (Table 2). Four patients experienced two or more anesthetic complications. Most complications occurred during general anesthesia, but the incidence of different complications was widely spread. Three patients experienced laryngospasms and two patients had to be reintubated. One patient had a respiratory depression, one patient had a low oxygen volume during surgery, and in one case the tube disconnected. Six other patients suffered from minor complications, such as tachycardia, high blood pressure, and patient reaction, which did not need intervention by the anesthesia team. In two cases, patient compliance was an issue.
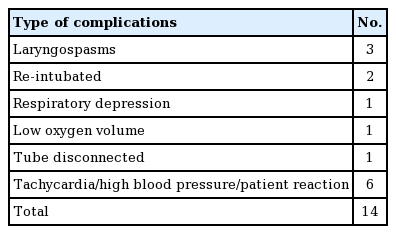
Anesthesia-related complications during surgery
The intraoperative and early postoperative complications following cleft lip and/or palate surgery were assessed (Table 3). In 26 cases, at least one surgical complication occurred. In 14 cases, excessive bleeding (hemorrhage) was seen, and in one of those cases the electrical hemostatic device failed. When bleeding was uncontrollable, but electrical hemostasis was not available, dabbing and pressurizing the wound bed with sterile gauze was time-consuming, but helpful.
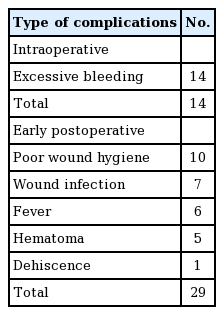
Intraoperative and early postoperative complications following cleft lip and/or palate surgery
Of the 98 operations, 69 (70%) were considered to have a flawless outcome at a 7-day follow-up appointment. Twenty-nine patients encountered an early postoperative complication, and four of them had at least two complications. In 10 cases, extremely poor wound hygiene was seen, and in seven of those cases the wound was infected. Additionally, three of these patients showed—along with poor wound hygiene and wound infection—distinct bleeding of the wound, even several days post-surgery.
Six patients had a fever during the 7 days of postoperative recovery, or at the time of their check-up. Five labioplasty patients suffered from a hematoma. In one case, dehiscence of the repair occurred post-labioplasty, possibly because rehabilitation instructions were not followed.
To summarize, a complication of any type occurred in 26 of the 66 (40%) labioplasty procedures, both revisions and primary, and a complication was seen in 22 of the 31 palatoplasty operations. Using the Pearson chi-square test, a significant difference was found in the complication rate between the procedure types (χ2=0.02; P<0.05). Of course, the effects of minor complications should be taken into consideration. Even though the incidence of complications overall showed a significant difference, no relationship was found between perioperative complications related to anesthesia and the occurrence of postoperative complications (χ2=1.00; P>0.05). Nonetheless, a significant difference was found between the procedure types regarding perioperative complications and the occurrence of postoperative complications (χ2=0.031; P<0.05). Because of the higher mean age of the patients treated in Indonesia, it is important to identify whether age is associated with any increase in the complication rate. However, no correlation was found between the incidence of complications and patients’ age (Fig. 4).
Complication rates by age group
DISCUSSION
In the previous literature, it has been reported many times that Indonesia has the most facial cleft patients per population worldwide [7]. The fact that Indonesian cleft surgery initiatives mainly focus on charity missions made it possible for the present study to observe numerous operations during 3 months in the east part of Indonesia. More than 100 patients received cleft surgery in only four charity trips. Patients were seen with a short intake (24 hours before surgery), and during surgery, intraoperative complications, both anesthetic and surgical, were assessed.
Unfortunately, the Indonesian medical system is not yet consistent in terms of patient documentation, making any type of research in the country challenging. Because the Indonesian population is not used to any type of bureaucracy, data collection is hard. For example, parents and/or caretakers often do not know their child’s date of birth or age. Managing treatment plans, appointments, costs, and patient data seems important to both doctors and their medical staff, so it appears that some form of data management is needed, especially when procedures (e.g., cleft surgery) are being performed on a large scale.
The ideal time for palate repair that can deliver good postoperative results is between 3 and 6 months of age [8,9]. Some researchers think that the age between 12 and 18 months is the best time for cleft repair [1], while others assume that patients who undergo palatoplasty surgery at the age of 1 year can have a significant improvement in speech. However, this timing of surgical treatment is uncommon in the rural areas of developing countries such as Indonesia, as patients still present with complications and visual defects during both adolescence and adulthood. The main reasons for this may include the late diagnosis of cleft deformities and the lack of resources for prompt management of cleft deformities.
Delays in surgery may be caused by financial barriers and non-financial barriers related to general life issues among rural populations [10]. Geographic, systemic, and individual characteristics have a clear relationship with and bearing on the receipt of timely care in rural areas [4,10]. A study conducted by Meara et al. [4] found that 5 billion people lack access to safe, affordable surgical and anesthetic care when needed. This problem is especially aggravated for the rural poor, as they must pay for both the medical costs and the expense of traveling and staying near the treatment center [10,11]. At least in some cases, patients along with their families travel from a rural/remote area to obtain the treatment where it is provided [6].
Schwarz and Bhai Khadka [11] found that the reasons for which patients often present to the surgeon at a very late time in developing countries include a lack of knowledge about treatment options, a lack of treatment services, and a lack of finances for treatment. Furthermore, Grimes et al. [12] mentioned that the structural barriers that contribute to difficulties in accessing surgical services in rural areas include a lack of facilities, cultural barriers, and financial shortages. All of these can lead to delays in the management of cleft lip and cause more risks and complications in cleft palate reconstruction. This fact seems to be consistent with the facts observed in rural areas of Indonesia.
The Lancet Commission on Global Surgery (2015) found that the human and economic consequences of untreated surgical conditions in LMICs are large and for many years have gone unrecognized [4]. The best solution for patients to access surgical and anesthetic care is multidimensional, encompassing geographic, temporal, structural, sociocultural, financial, and political components. Patients should then be able to access this system in a timely manner [4]. The Indonesian government announced in 2014 that it is preparing plans for a public health care system that should provide cleft surgery for most patients who cannot afford cleft surgery on their own. Perhaps this step could also provide a framework for measures addressing handicaps of data management, consultations, and infrastructure. In that way, hopefully cleft operations could be performed in earlier stages of infancy.
In the present study, a total of 112 patients presented for cleft surgery at the charity missions that took place in the 3 months covered by this study. This underscores the large number of cleft patients in Indonesia and the continuous desire for help. However, a significant number of minor and major complications were encountered during and after surgery. Overall, the anesthetic, surgical, and postoperative complications were found to be significant.
Most palatoplasty complications occurred during general anesthesia, specifically tachycardia and high blood pressure that led to a patient reaction. However, those cases did not require intervention by the anesthesia team. In a previous study, Fillies et al. [13] stated that the likelihood of risks and complications during general anesthesia for cleft lip repair and palatoplasty is three times higher in children than in adults.
The study conducted by Fillies et al. [13] revealed that blood loss is a frequent complication that may be attributed directly or partially to intraoperative factors. Accordingly, in our study, we found that the most frequent complications included excessive bleeding (hemorrhage) and in one such case, the electrical hemostatic device failed. This complication especially affects patients intraoperatively before extubation and when they are in the recovery room [14]. In order to minimize the total blood loss, shortening the duration of cleft surgery is an important factor [13]. However in complex repairs, the operation may be longer and can require more dissection, which increases the risk of bleeding, swelling, and elevated postoperative pain levels [15].
Of the 98 surgical procedures that were analyzed in our study in relation to early postoperative complications, serious issues included extremely poor wound hygiene, wound infection, and dehiscence of the repair, possibly due to a lack of following rehabilitation instructions. This is similar to a previously published report finding that wound dehiscence was the major post-palatoplasty complication in 14 patients [16]. Cohen [17] found that dehiscence and fistulas were complications requiring correction in additional surgery after palatoplasty. Aziz et al. [8] reviewed their experiences during multiple cleft surgical missions in rural Bangladesh, and the 2007 mission in particular showed that six pediatric patients developed postoperative infections with associated wound dehiscence.
The present study was limited to east Indonesia, and further studies related to cleft lip and palate surgery are therefore still required at other health centers in Indonesia. In addition, the short follow-up period (only 7 days) is another weakness of this study, as sometimes it takes longer in the healing process for certain complications to develop. However, the analysis in this report provides important data for improving the treatment plans for cleft lip and palate surgery. Long-term postoperative results need to be assessed to give a vital estimation of the success of cleft strategies in Indonesia and to evaluate any improvements that are made in the near future. The expectation is that the appeal of (early) cleft surgery will only grow in the following years. Therefore, complementary research with a larger group of patients is recommended to involve more of the Indonesian population in the results.
The overall rate of complications of cleft lip and palate surgery in rural areas of Indonesia was significant. However, there was no correlation between the incidence of complications and patients’ age, which is an important finding since the mean age of the patients was high. The significant complication rates and fluctuating surgical outcomes presented in this study illustrate that improvements in cooperation and collaboration are needed in several important disciplines in Indonesian cleft care. Therefore, it is important that ongoing changes and improvements are evaluated in further studies in the near future.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Health Research Ethics Committee of the Hasanuddin University (approval number: UH14060319) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consents were obtained.
Patient consent
The patients provided written informed consent for the publication and the use of their images.
Author contribution
Conception and design of the study, acquisition of data, and analysis and interpretation of data: Ruslin M, Dom L, Thamrin SA. Drafting the article or revising it critically for important intellectual content: Tajrin A, Yusuf ASH, Arif SK. Final approval of the version to be submitted: Tanra AH, Ou KL, Forouzanfar T, Thamrin SA.