Dermatofibrosarcoma Protuberans with Pulmonary Metastasis in the Absence of Local Recurrence
Article information
Dermatofibrosarcoma protuberans (DFSP) is a relatively unusual fibrohistiocytic tumor that is classified as an intermediate-grade malignancy [1,2]. DFSP is characterized by infiltrative growth and a high propensity for local recurrence after surgical excision [1-4]. Despite its locally aggressive behavior, DFSP has little metastatic potential [1-4], and when distant metastasis does occur, it almost always arises after repeated local recurrences and usually involves lung, bone, or locoregional lymph nodes [1,3,4]. The authors report a rare case of a DFSP that metastasized to the lung without any preceding local recurrence.
A 32-year-old otherwise healthy woman presented with a 1×1 cm sized, well-circumscribed, skin-colored maculopapular lesion of one year's duration on the anterior aspect of her right thigh. Histopathologically, the excised tumor was composed of spindle-shaped cells, which were positive for CD34 and were arranged in a storiform pattern (Fig. 1A). Focal fibrosarcomatous changes presented in a herringbone pattern and were associated with CD34 negativity (Fig. 1B). Cellularity and mitotic activity were much higher (10/HPF) in the fibrosarcomatous than in the DFSP areas. No distant metastasis was detected preoperatively by pelvic computed tomography or positron emission tomography (PET). Wide excision with a 3-cm free margin, including the deep fascial layer, was performed; the resulting defect was reconstructed with a fasciocutaneous flap. Subsequently, regular evaluations were undertaken for local recurrence and distant metastasis.

Histopathologic findings of the right thigh mass. (A) The junction between the dermatofibrosarcoma protuberans (DFSP) and the fibrosarcomatous component is indicated by black arrows. The area on the lower left with lower cellularity is the DFSP portion and the upper right area with higher cellularity is the fibrosarcomatous dermatofibrosarcoma (FS-DFSP) portion (H&E, ×100). (B) DFSP shows strong immunoreactivity in the lower left of the photomicrograph, and the FS-DFSP region shows weak immunoreactivity in the upper right. The boundary between DFSP and FS-DFSP is indicated by black arrows (CD34, ×100).
Three years after surgery, PET computed tomography (CT) was performed for a routine evaluation of recurrence and metastasis, without any symptoms or signs. Multiple pulmonary nodules were found on PET CT and a subsquent lung CT scan revealed the same results (Fig. 2). The CT-guided biopsy specimen of the lung was histopathologically and immunohistochemically identical to the tumor previously resected from the thigh (Fig. 3). These findings resulted in a diagnosis of metastasis. Subsequently, the patient was treated with multiple chemotherapeutic agents, including adriamycin, dacarbazine, and ifosfamide. Four years after the metastasis was discovered, there was no evidence of disease progression and and the disease exhibited stability.
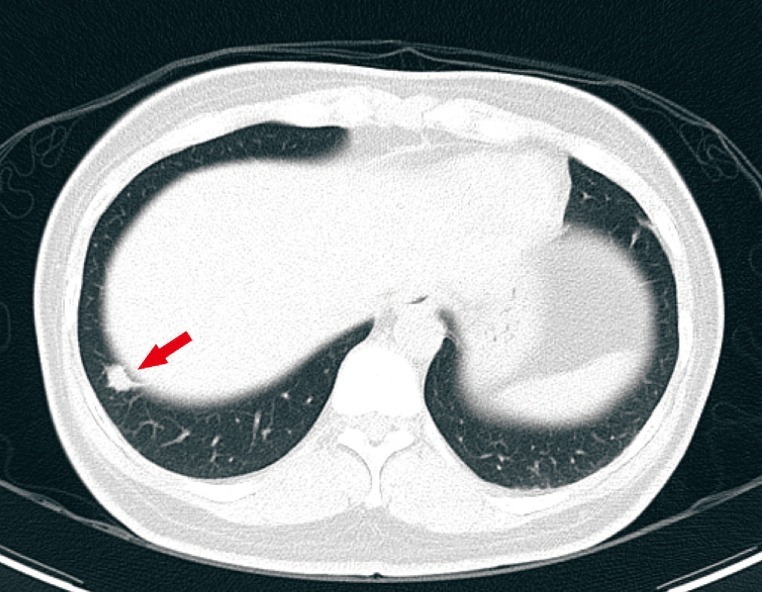
Computed tomographic images of the lungs. Three years after surgery, multiple pulmonary nodules (red arrow) were noted by CT.
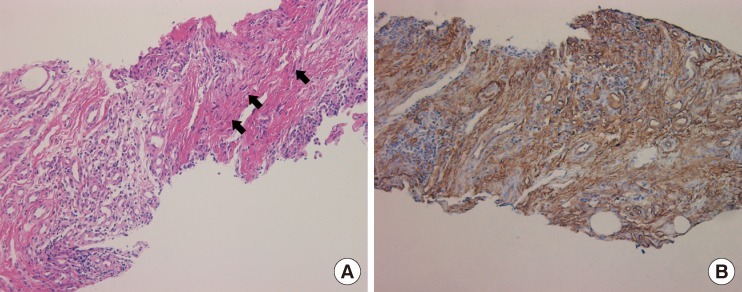
Histopathologic finding of the lung nodule. (A) The specimen of the lung biopsy shows infiltration of multiple spindle cells arranged in a storiform pattern (black arrows), identical to the tumor previously resected from the thigh (H&E, ×100). (B) The diffuse brown staining of the tumor cells in the lung nodule[s] shows the presence of CD34 (CD34, ×100).
DFSP is a fibrohistiocytic tumor of intermediate-grade malignancy with locally aggressive and infiltrative capabilities [1-4]. It has an incidence of only 3-6.5 cases per million persons per year, and usually arises during early to middle age [4]. DFSP is typically found on the trunk, proximal extremities, head, and neck, but may present at almost any site [1,2]. Furthermore, DFSP is characterized by a high propensity for local recurrence. According to previous articles, about 11% to 53% of affected patients experience relapse after adequate wide excision, and the local recurrence rate was affected by the depth of disease invasion, site of disease, high mitotic activity, microscopically close resection margin, and increased cellularity [5]. However, despite this high frequency of local recurrence, metastasis only occurs in less than 6% of cases [4]. Metastasis mostly occurs after repeated local recurrences and most commonly in lung, bone, and locoregional lymph nodes [1,3,4]. On the other hand, distant metastasis without local recurrence is rare; our review of the literature revealed only three other reported cases [1-3]. Systemic evaluation is needed for the early diagnosis and proper management of patients with distant metastasis in the absence of local recurrence.
A more hostile subtype of DFSP presents with fibrosarcomatous transformation, and is called 'fibrosarcomatous dermatofibrosarcoma (FS-DFSP)' [1,4]. Regions of fibrosarcomatous progression are characterized by a herringbone growth pattern, dense cellularity, a greater proportion of atypical cells, large cell sizes, and increased mitotic activity [4]. Furthermore, FS-DFSP shows remarkably diminished or absent CD34 immunoreactivity [1,4]. This condition is considered a progressed form of DFSP with increased metastatic potential [1,4], and it has been reported that old age, dense cellularity, high mitotic index (more than 10 mitotic figures/HPF), a microscopically close resection margin, and specific histopathologic subtypes, such as, FS-DFSP, have a poor prognosis [1]. These findings caution that more careful local and systemic evaluations are needed in patients with a history of hostile histopathologic results, especially in cases of FS-DFSP.
Although DFSP has little metastatic potential, and it almost always arises after repeated local recurrences, we suggest that more careful local and systemic evaluations are needed for the early diagnosis and proper management of patients with distant metastasis in the absence of local recurrence, especially in cases of more hostile histopathologic results.
Notes
This article was presented as a poster at the 1st Research & Reconstructive Forum on May 12-13, 2011 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.