Relationship between Locations of Facial Injury and the Use of Bicycle Helmets: A Systematic Review
Article information
Abstract
The aim of this study is to review the protective effect of a bicycle helmet on each facial location systematically. PubMed was searched for articles published before December 12, 2014. The data were summarized, and the odds ratio (OR) between the locations of facial injury was calculated. A statistical analysis was performed with Review Manager (The Nordic Cochrane Centre). Bicycle helmets protect the upper and middle face from serious facial injury but do not protect the lower face. Non-wearers had significantly increased risks of upper facial injury (OR, 2.07; P<0.001) and of middle facial injury (OR, 1.97; P<0.001) as compared to helmet users. In the case of lower facial injury, however, only a slightly increased risk (OR, 1.42; 95% confidence interval (CI), 0.67-3.00, P=0.36) was observed. The abovementioned results can be attributed to the fact that a helmet covers the head and forehead but cannot cover the lower face. However, helmets having a chin cap might decrease the risk of lower facial injury.
INTRODUCTION
Previous studies have reported that wearing a bicycle helmet reduces the risks of facial injury and head injury [123].
However, there are few papers that provide the ratio of people who wear a bicycle helmet and the incidence of injury. In fact, a previous study reported that bicycle helmets could reduce the risk of injury in the upper and middle facial region but provided no protection to the lower facial region [45].
The aim of this study is to review the protective effects of a bicycle helmet on each facial location systematically.
METHODS
For helmet use and location of facial injury, the search terms "facial trauma OR facial injury OR facial location" AND "helmet OR bicycle helmet OR cycling helmet OR head protective device" were used in a PubMed search, which resulted in 417 papers (Fig. 1).
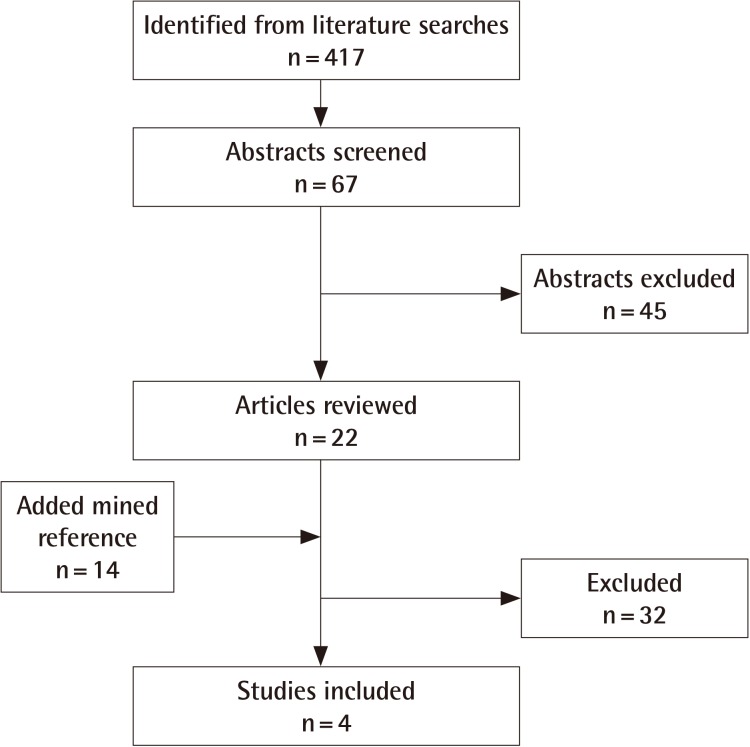
Literature flowchart for this study
Literature flowchart for helmet use and location of facial injury.
Studies that did not include an evaluation of the relationship between bicycle helmet use and the location of any facial injury were excluded. No restrictions on language and publication forms were imposed. All the articles were read by two independent reviewers who extracted data from the articles.
The data were summarized and the odds ratio (hereafter, OR) between the locations of facial injury were calculated. A statistical analysis was performed with Review Manager (The Nordic Cochrane Centre).
RESULTS
Among the 417 titles, we found 22 potentially relevant articles, from which 4 papers met our inclusion criteria (Fig. 1).
Helmet use and location of facial injury
Upper facial injury vs. non-facial injury
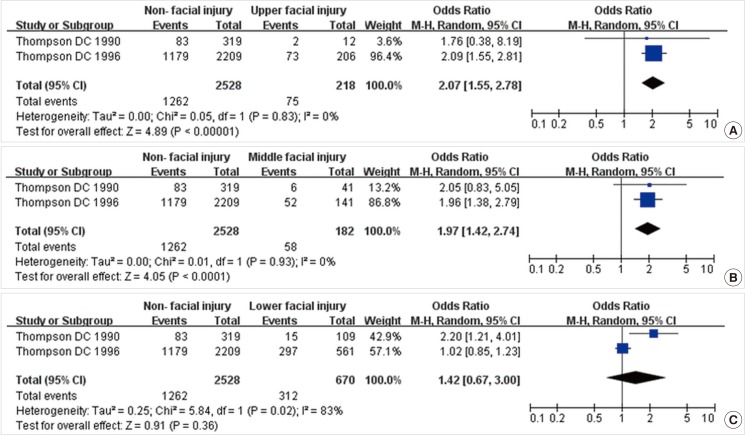
Two studies were sub-grouped, and a meta-analysis of their data suggested that there is a significantly increased risk of upper facial injury (except abrasions or contusions) for non-users as compared to helmet users (n=2,836; OR, 2.07; 95% confidence interval [CI], 1.55-2.78; Z=4.89, P<0.001, heterogeneity: chi2=0.05, I2=0%) (Table 1, Fig. 2A) [45].

Helmet use and location of facial injury
Helmet use and location of facial injury
(A) Upper facial injury versus non-facial injury, (B) Middle facial injury versus non-facial injury, (C) Lower facial injury versus non-facial injury.
Middle facial injury versus non-facial injury
Two studies were sub-grouped and a meta-analysis of their data suggested that there is a significantly increased risk of middle facial injury in non-users as compared to helmet users (n=2,710, OR=1.97, 95% CI=1.42-2.74, Z=4.05, P<0.001, heterogeneity: Chi2=0.01, I2=0%) (Table 1, Fig. 2B) [45].
Lower facial injury versus non-facial injury
Two studies were sub-grouped and a meta-analysis of their data suggested that there is a slightly increased risk of lower facial injury in non-users as compared to helmet users (n=3,198; OR, 1.42; 95% CI, 0.67-3.00; Z=0.91; P=0.36; heterogeneity, Chi2 =5.84, I2=82%) (Table 1, Fig. 2C) [45].
DISCUSSION
Facial injury occurs in 43 out of 100,000 accident cases in the United States [4]. In the present study, the facial protection effect of a helmet varied according to the face location analyzed.
Non-users had a significantly increased risk of upper facial injury (OR, 2.07; P<0.001) and of middle facial injury (OR, 1.97; P<0.001) as compared to helmet users. In the case of lower facial injury, however, only a slightly increased risk (OR, 1.42; 95% CI, 0.67-3.00; P=0.36) was observed. In other words, bicycle helmets protect the upper and middle face from serious facial injury but not the lower face.
The abovementioned result can be attributed to the fact that a helmet typically covers the head and forehead but does not cover the lower face. Further, despite the fact that most helmets cannot directly protect the middle face, we observed that the risk of middle facial injury could be reduced significantly by wearing a helmet (OR=1.97, P<0.001). This observation could be attributed to the following: first, because the helmet peak changes the angle of the second impact, when the rider is falling down, the helmet that covers the head and upper face comes into contact with the ground before the middle face (Fig. 3). Second, since the helmet directly protects the upper face, the severity of the nearby middle face injury could also be lowered by wearing a helmet.

Middle face protecting effect of the helmet
Mechanism of the middle face protecting effect of the helmet. When the rider falls down, the helmet peak (P) comes into contact with the ground before the middle face.
Further, we agree with Thompson et al. [4] and Acton et al. [6] that wearing a helmet having a chin cap might decrease the risk of lower facial injury.
The facial injuries that Acton et al. [6] and Lima et al. [7] considered were classified as upper, middle, and lower. However, we could not find a control group in Lima's paper nor could we find helmet use as a percentage in Acton's paper [67]. Therefore, we could not consider these two papers in the meta-analysis.
In conclusion, bicycle helmets protect the upper and middle face from serious facial injury but not the lower face.
Notes
No potential conflict of interest relevant to this article was reported.