Lymphoepithelioma-like Carcinoma of the Skin in the Cheek with a Malignant Metastatic Cervical Lymph Node
Article information
Since first described by Swanson et al. in 1988, lymphoepithelioma-like carcinoma of the skin (LELCS) has been considered a rare malignant skin tumor. It is usually caused by sun exposure and is therefore most prevalent on the skin of the head and neck in elderly individuals. Although the histologic etiology of LELCS is still unclear, it is known to have a slight tendency toward local recurrence and extremely low metastatic potential. Approximately 70 cases have been reported in the literature to date [1]. Among them, only a few reports have described local recurrence or metastasis to lymph nodes, and only one reported death due to distant metastasis of LELCS. In Korea, two LELCS cases have been reported in the Korean language. However, both cases had no local recurrence or lymph node metastasis nor any long-term follow-up data. We report the first case of LELCS with a malignant metastatic cervical lymph node in a Korean. A 71-year-old male with a skin lesion of the right cheek, which appeared several months prior to presentation, visited our hospital. Clinically, the lesion presented as soft, mobile over the underlying tissues, and painless, with a diameter of 5 mm and an erythematous macule with central eschar caused by a punch biopsy at an another hospital (Fig. 1). He did not have any palpable lymphadenopathy or nasopharyngeal symptoms. The slide from the other hospital was re-evaluated in our hospital; poorly differentiated carcinoma was identified in the dermis. Magnetic resonance imaging (MRI) showed a focal defect lesion approximately 5 mm in size surrounding the enhancement with an ambiguous impression suggesting either tumor enhancement or a post-biopsy reaction (Fig. 2), and a whole-body positron emission tomography (PET) scan showed skin thickening with focal hypermetabolism in the right cheek. In ultrasonography (USG), palpable and abnormal lymph nodes were not observed. Surgical treatment was performed with wide excision (surgical margin, 1 cm) and reconstruction with a local bilateral advancement flap (Fig. 3). Five sites of the resection margin were checked intraoperatively by frozen biopsy, and all of the results were negative. Histopathologic assessment revealed a poorly differentiated carcinoma, with a dense lymphoplasmacytic infiltration; neither lymphovenous nor perineural invasion was identified (Fig. 4). Positive staining was observed with cytokeratin 7, cytokeratin 5/6 (CK 5/6), androgen receptor, Ki-67, P63, and vimentin (Fig. 5). Conversely, the cancer cells were negative for GCDFP-15, S-100, and Epstein-Barr virus (EBV). The patient did not undergo additional postoperative treatment, such as chemotherapy, radiation, or zinc chloride fixative. After 4 months, a new palpable lesion was identified in the right side of the patient's neck. An enlarged lymph node, approximately 1.1 cm in size, was discovered via computed tomography (CT) at the right level IB with an inner necrotic portion, which suggested metastatic lymphadenopathy (Fig. 6). Therefore, the patient underwent a type-3 modified radical neck dissection. A total of 36 lymph nodes were obtained, and only one level IB lymph node was identified as a metastatic carcinoma. After the pathologic result was reported, the patient was referred to a radiation oncologist and received radiation therapy (60.75 GY) in the cheek and right neck area for 2 months. The patient recently has completed his postoperative clinical follow-up of 1 year and 8 months, and there were no clinical and radiological findings that suggested local recurrence or distant metastasis.

Preoperative photograph of the patient. An erythematous macule with central eschar (red arrow) can be observed in right cheek.

The axial view of a T1-weighted magnetic resonance image showing a focal defect (red arrow) approximately 5 mm in size. The lesion is limited to the subcutaneous layer. It is not involved in the deep muscular structure or superficial dermal layer.

Intraoperative photographs of the patient. Wide excision is performed with a 1-cm surgical margin. For coverage of the defect after wide excision, a bilateral local advancement flap was used with bilateral dog-ear correction.
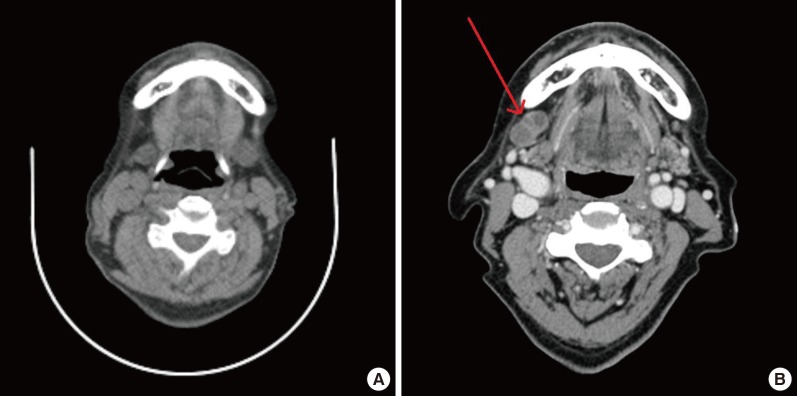
(A) The preoperative neck computed tomography (CT) scan, which had been taken at another hospital. No enlarged cervical lymph node can be seen. (B) The neck CT taken at postoperative four months showing an enlarged lymph node at right level IB with an inner necrotic portion that suggests metastatic lymphadenopathy.
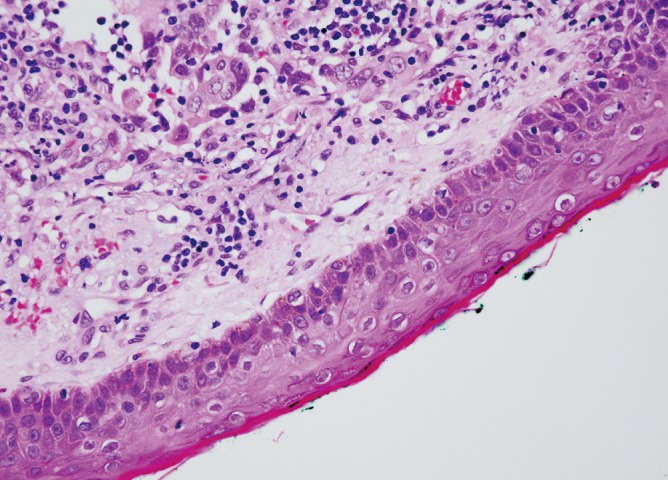
Tumor cells showing a rich quantity of eosinophilic cytoplasm, large pleomorphic nuclei, and prominent nucleoli. Intradermal tumor expansion up to the papillary dermis without epidermal ulceration (H&E, 200).
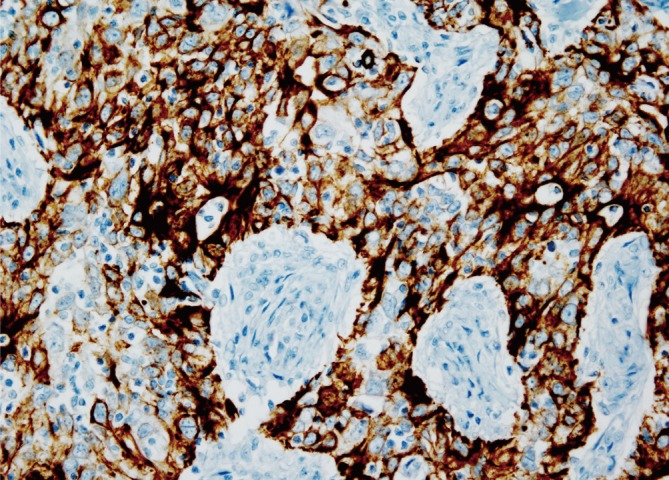
Cytokeratin 5/6 is very useful in detecting squamous differentiation. Lymphoepithelioma-like carcinoma represented a poorly differentiated variant of squamous carcinoma, so cytokeratin 5/6 can be used as a confirmatory immunostain. In the figure, neoplastic epithelioid cells with expression of cytokeratins can be seen (CK 5/6, ×200).
LELCS is a very rare cutaneous neoplasm, with an annual incidence of 1 per 100,000. LELCS typically presents as a slowly growing flesh-colored or erythematous firm nodule, papule, or plaque [2]. LELCS is positive for high molecular-weight cytokeratins, such as pancytokeratin and epithelial membrane antigen, on immunohistochemical staining, which indicates the epithelial origin of the neoplastic cells. The surrounding inflammatory cells stain with the T-cell marker CD3 and B-cell marker CD20. In addition, LELCS shows a strong reactivity for p63 protein, CK5/6, and CAM5; on the other hand, immunostaining for carcinoembryonic antigen, S-100 protein, CK-20, CK-7, and NSE is always negative [3]. Only one case of EBV-positive LELCS has been reported, in a tumor from the cheek of a Japanese woman; as in our case, LELCS is typically found to be negative for the EBV. A differential diagnosis should be considered since LELCS has similar histological features with metastatic nasopharyngeal carcinoma (NPC) and lymphoepithelioma-like carcinoma that occurs in other anatomic sites, such as the salivary glands, tonsils, larynx, thyroid, thymus, lungs, stomach, breasts, and uterine cervix [2]. The nasopharynx of patients should be examined to rule out metastasis from NPC. Because NPC is positive for the EBV, polymerase chain reaction or in situ hybridization testing is reliable for differentiation. Lymphoepithelioma-like carcinoma (LELC) of the stomach, salivary gland, lung, and thymus is also known to be associated with EBV infection [4]. It is important to rule out metastasis from primary LELC of the listed organs. Many treatment techniques for LELC have been accepted, including electrocauterization, curettage, Mohs micrographic surgery, wide excision, radiation therapy, chemotherapy, and adjunctive use of zinc chloride fixative. Above all, wide excision is considered to be the treatment of choice. Although no consensus on the best surgical margin has emerged, a 1-cm margin is most widely used. We chose a centimeter as the surgical margin, but cervical lymph node metastasis still occurred. Therefore, we believe that additional research is needed to determine the best surgical margin. Radiation therapy is effective because LELC has a great histological similarity to radiosensitive NPC. Despite its effectiveness, radiation therapy is reserved for local recurrence or lymph node metastasis because surgical resection is sufficient in most cases [5]. In conclusion, we report the first Korean case of LELCS in the cheek with a malignant metastatic cervical lymph node. As is well known, LELC has a relatively good long-term prognosis, but this case has an uncommon advanced presentation with cervical lymph node metastasis. However, although this case has the limitation of a relatively short follow-up, with surgical resection and adjuvant radiation therapy, it is possible that our patient could have maintained a recurrence-free status.
Notes
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (R11-2005-065).
This article was presented at the 71st International Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 1-3, 2013 in Seoul, Korea.
No potential conflict of interest relevant to this article was reported.