Intraneural Venous Malformations of the Median Nerve
Article information
Abstract
Venous malformations arising from the peripheral nerve are a rare type of vascular malformation. We present the first case of an intraneural venous malformation of the median nerve to be reported in a child and review the previous two cases of median nerve compression due to a venous malformation that have been reported. These cases presented with painless masses in the volar aspect of the wrist or with symptoms suggestive of carpal tunnel syndrome. Clinical suspicion should lead to the use of Doppler ultrasonography as the first-line diagnostic tool. Magnetic resonance imaging and histopathology can confirm the diagnosis, as phleboliths are pathognomonic of venous malformations. Surgical treatment appears to be the only modality capable of successfully controlling the growth of an intraneural malformation. Sclerotherapy and radiotherapy have never been used to treat this type of malformation.
INTRODUCTION
Venous malformations arising in peripheral nerves are a rare type of vascular malformation, and rarely origínate from the vasa nervorum. Only one case of intraneural venous malformation of the median nerve has been reported in the literature [1]. A case reported by Muchemwa et al. [2] involved an intramuscular venous malformation that led to extrinsic compression of the median nerve. Both cases presented with the symptoms of carpal tunnel syndrome. We present the first case of an intraneural venous malformation of the median nerve to be reported in a child.
CASE REPORT
A two-year-old male presented to our department with a palpable asymptomatic mass in his right palm that was present at birth and had subsequently exhibited a slow and steady pattern of growth (Fig. 1). Imaging showed the typical features of venous malformations [3]. Doppler ultrasonography indicated the presence of an irregularly shaped space-occupying lesion with multiple chambers and a low level of blood flow between the flexor retinaculum and the external flexor tendons, next to the branch of the nerve innervating the thumb and index finger, and magnetic resonance imaging (MRI) showed a heterogeneous signal, with hyperintensity on T2-weighted imaging and after gadolinium administration, and hypointensity on T1-weighted imaging.
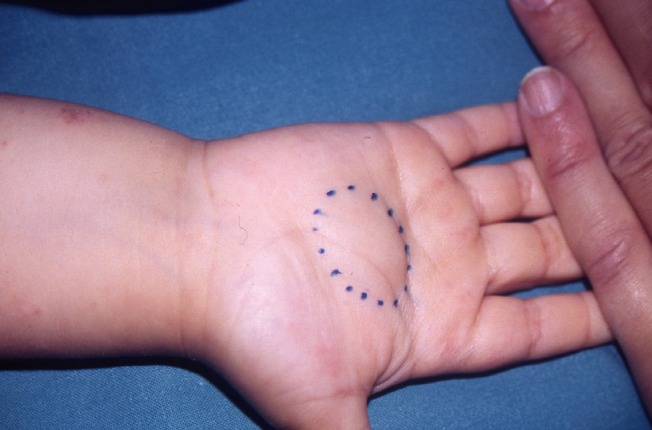
Preoperative frontal view of the mass
The extent of the tumor is defined by a discontinuous line.
It was decided to excise the mass in order to verify the diagnosis of a vascular malformation, and to control the growth of the tumor. Surgery showed a purple mass that was 2.5 cm long (Fig. 2), and interfascicular microdissection of the median nerve was required; nevertheless, neither nerve grafts nor sacrificing any fascicle was necessary. Despite the performance of internal neurolysis, neither sensory nor motor symptoms were observed in the postoperative period.
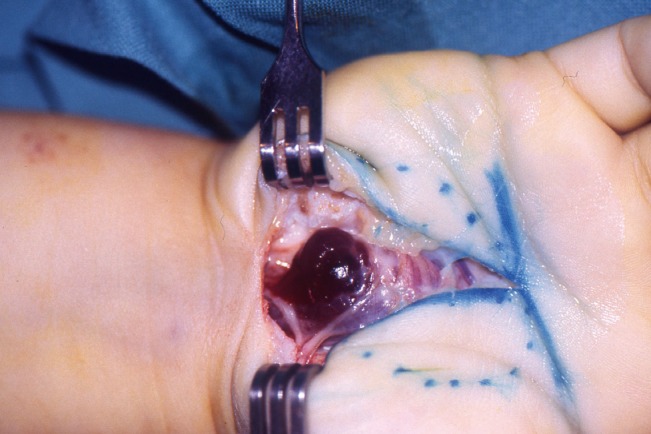
Intraoperative view
The surgical approach consisted of a longitudinal incision along the palm of the right hand, which revealed a purple mass that was carefully dissected from the superficial tendinous fascicles. Interfascicular microdissection of the median nerve required optic magnification and was performed under limb ischemia.
Histopathological analysis revealed ectatic channels, surrounded by a thin layer of endothelial cells without hyperplasia (Fig. 3). Immunostaining with GLUT-1, WT-1 and D2-40 was negative. These results were compatible with a venous malformation.
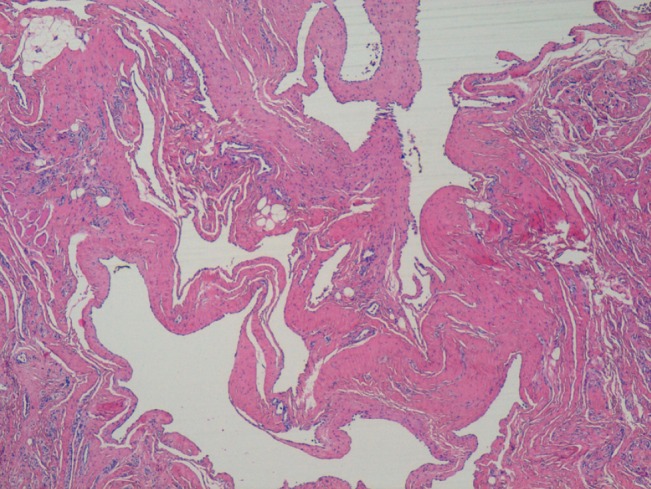
Cross section of the mass
Microscopic histopathology demonstrated the presence of multiple ectatic channels, surrounded by a thin layer of endothelial cells without hyperplasia (H&E, ×400).
A year after the intervention, the patient presented to our department with a local relapse. No sensory, motor, or electromyographic deficiencies were found. The mass continued to grow steadily and after 10 years of follow-up, the patient reported local pain and numbness in the thumb, index, middle and ring fingers, and a new operation was planned.
The reintervention revealed a bluish irregular mass (Fig. 4), that was 7 cm long and surrounded and infiltrated the median nerve. The histopathology results were the same as those obtained after the first operation; however, this time phleboliths were found (Fig. 5), confirming the diagnosis of venous malformation. Phleboliths and calcifications, pathognomonic of venous malformations, can be found after episodes of local intravascular coagulation, if the venous malformations are medium to large in size [3]. This may have been the reason why they appeared in the surgical specimen from the second intervention (7.5 cm in length), but not in the surgical specimen from the first operation (2.5 cm).

Reintervention intraoperative view
Intraoperative view of the second operation showing a bluish irregular mass, measuring 7×2.5×1.5 cm, which surrounded and infiltrated the median nerve, affecting the interfascicular space from the distal third of the forearm to the distal palmar crease, above the metacarpophalangeal joints.

Surgical specimen in the reintervention
Surgical specimen from the second operation, consisting of the venous malformation and four phleboliths, pathognomonic of a venous malformation.
Although macroscopic complete excision seemed to be achieved, a new local relapse was clinically detected and confirmed by MRI 12 months subsequently (Fig. 6).
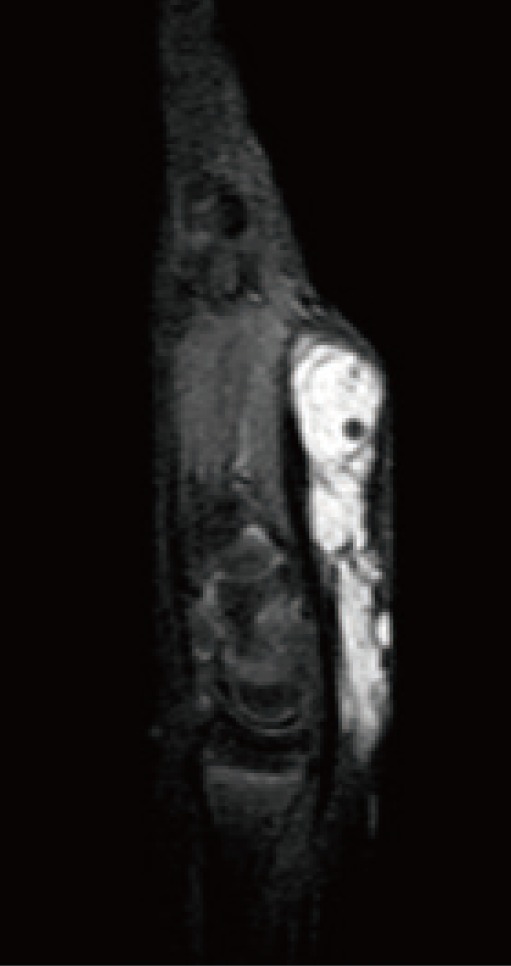
Magnetic resonance imaging of the relapse
Of particular note is the hyper-intense signal of the mass on the T2-weighted sequence, with the mass located between the flexor retinaculum and the external flexor tendons in the wrist and extending from the distal third of the forearm to the distal palmar crease.
DISCUSSION
The standard of care for intraneural venous malformations requires a multidisciplinary approach and a thorough assessment of the location and extension of the lesion.
Sclerotherapy, laser therapy (neodymium), cryotherapy and pressure therapy are possible alternatives for venous malformations affecting other structures, but have never been used to treat intraneural malformations.
With regard to intraneural venous malformations, surgery is the only treatment modality capable of controlling growth and compressive symptoms, although it was a temporary solution in the case presented in this report due to relapse after 12 months after the first and second operations [4]. In the case reported by Hariri et al. [1] no relapse took place over 12 months of follow-up. It is possible to avoid potential surgical difficulties, such as the tendency towards bleeding due to the vascular richness of the malformed tissue, by employing meticulous surgical techniques, using optical magnification and limb ischemia. Postoperative complications did not occur in any of the three cases.
Notes
We would like to thank Marta Gago Pesado for reviewing the translation of the manuscript, and Rose Hernández Cancela for providing us with the histopathological images.
No potential conflict of interest relevant to this article was reported.