Immediate Bilateral Breast Reconstruction with Unilateral Deep Superior Epigastric Artery and Superficial Circumflex Iliac Artery Flaps
Article information
Abstract
Autologous breast reconstruction utilizing a perforator flap is an increasingly popular method for reducing donor site morbidity and implant-related complications. However, aberrant anatomy not readily visible on computed tomography angiography is a rare albeit real risk when undergoing perforator flap reconstruction. We present an operative case of a patient who successfully underwent a bilateral breast reconstruction sourced from a unilateral abdominal flap divided into deep superior epigastric artery and superficial circumflex iliac artery flap segments.
INTRODUCTION
Bilateral breast reconstruction from abdominal perforator flaps has increased in frequency and popularity in recent decades while these flaps' advantages continue to be well documented in the literature [1]. The vascular supply to these flaps is often variable and differs in location, size, and course [2]. It was previously theorized that a history of abdominal surgeries in a patient limits the ability to utilize the transverse rectus abdominis myocutaneous and deep inferior epigastric perforator (DIEP) flaps in reconstruction. Recent reports, however, have demonstrated that abdominal wall scars including the Pfannenstiel scar are not a contraindication with appropriate planning and flap design [34].
CASE
A 41-year-old woman with locally advanced right breast cancer presented for bilateral DIEP flap breast reconstruction (Fig. 1). She had undergone lumpectomy with positive margins followed by completion mastectomy with tissue expander placement and subsequent radiation therapy. An autologous reconstruction was desired, and her abdominal wall was considered as a source. She had undergone a total abdominal hysterectomy ten years previously, following three prior cesarean sections. Preoperative computed tomographic angiography (CTA) demonstrated several bilateral periumbilical deep inferior epigastric artery perforators of adequate size and location. Intraoperatively, we raised the right hemi-abdominal flap to find that the right superficial inferior epigastric artery and deep inferior epigastric artery (DIEA) were encased in fibrotic tissue. Further dissection demonstrated the right deep superior epigastric artery (DSEA) and superficial circumflex iliac artery (SCIA) of inadequate caliber (a size mismatch of approximately 1 mm in diameter) for microanastomosis, leaving the right hemiflap insufficient for free tissue transfer. The left DIEA was similarly surrounded by fibrotic tissue and of insufficient caliber.

Preoperative photograph
Preoperative photograph of a 41-year-old with right breast cancer before bilateral mastectomy.
Intraoperatively, the deep inferior epigastric vessels were interrupted with scar tissue at approximately 2 cm from the origin of the main perforators. Fig. 2 on the preoperative CTA demonstrates the proximal left DIEA with a decrease in caliber with complete reconstitution of the vessels past this area of stenosis.
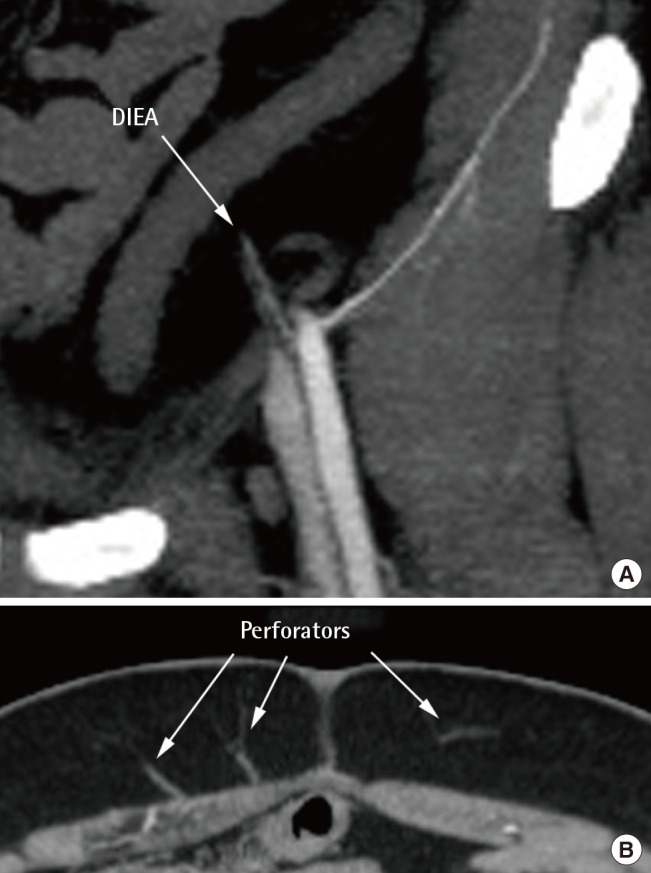
Computed tomographic angiography
Coronal section of the left proximal deep inferior epigastric artery (DIEA) (A) and axial section of the perforators (B). Computed tomographic angiography acquisition settings: 1-mm source images in the axial plane after intravenous injection of Isovue 370 on a Phillips Multidetector computed tomography, using a bolus tracking technique with the region of interest placed on the aortic arch to ensure accurate bolus timing. Post-processing was completed in three planes (axial, coronal, and sagittal) with multiplanar reconstruction and 3D maximum intensity projection during the arterial phase.
As a consequence of the aberrant anatomy, we designed two flaps for bilateral breast reconstruction from the left hemi-abdominal tissue in situ (Fig. 3) utilizing the SPY Elite perfusion assessment instrument (Novadaq Technologies, Ontario, Canada; LifeCell, Branchburg, NJ, USA). The left DSEA was initially microanastomosed to the right internal mammary artery. After successful right breast microanastomotic completion, the left hemiabdominal flap was divided (Fig. 4). Subsequently, we performed the microanastomosis of the left SCIA to the left internal mammary artery followed by bilateral flap inset (Fig. 5).
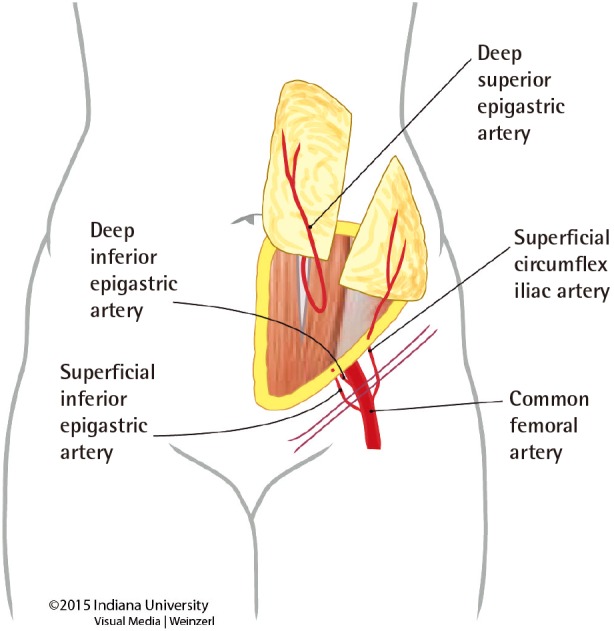
Schematic illustration of flap elevation
Illustration of the left hemi-abdominal flap split based on the arterial supply of the deep superior epigastric and superficial circumflex iliac arteries.
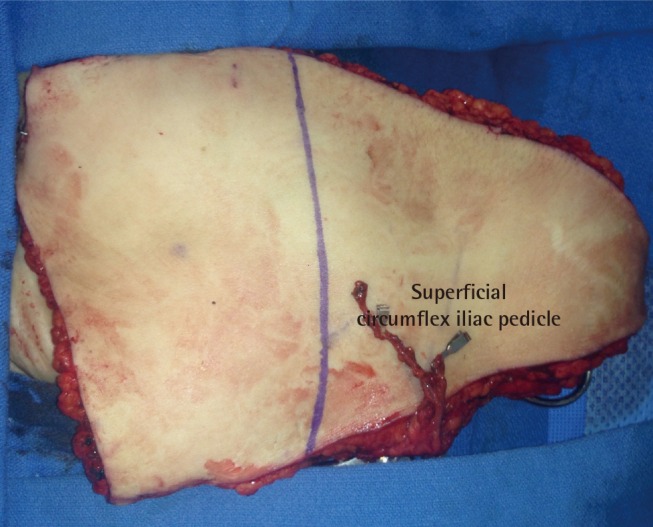
Intraoperative photograph
Intraoperative photograph showing the planned division of the left hemi-abdominal flap after microanastomosis of the left deep superior epigastric artery to the right internal mammary artery.

Intraoperative photograph
Intraoperative photograph of the completed inset of the deep inferior epigastric artery (right breast reconstruction) and superficial circumflex iliac artery (left breast reconstruction) flaps.
Postoperatively, much less tissue volume was transferred than originally planned. We did not go directly to implant reconstruction because of the autologous tissue reconstruction desired by the patient and knowing her history of radiation therapy. The patient agreed that increased volume and improved symmetry was needed for optimizing her aesthetic outcome. Three months postoperatively, 150 mL and 225 mL high profile silicone implants were placed beneath the DSEA flap (right reconstructed breast) and SCIA flap (left reconstructed breast), respectively (Fig. 6). Implant placement was optimal for enhanced projection with excellent coverage beneath the perforator flaps. Implant placement beneath DIEP flap breast reconstruction has been previously described [5] and helps achieve symmetry while offering superior tissue coverage over an implant in a radiated field.

Three months postoperative photograph
Outcome after placement of high profile silicone implants beneath the autologous perforator flap breast reconstruction.
DISCUSSION
CTA has emerged as a key preoperative tool in surgical planning of perforator flaps, allowing for the precise identification of dominant perforators while reducing operating time and complications [6]. The anatomic accuracy of abdominal wall CTA has been found to have a sensitivity of 96%–100% and specificity of 95%–100% in clinical and cadaveric studies [789]. Recent studies have further shown the superiority of CTA compared with Doppler and duplex ultrasounds [1011]. While these studies have proven the accuracy of CTA in determining perforator position, information about the caliber and adequacy of a perforator remains lacking. Intraoperative inspection of planned perforators has often found them to be less robust than on imaging and insufficient for transfer. In evaluating the clinical utility of CTA in DIEP free flaps, Keys et al. [12] noted the importance of surgical judgment in selecting perforators and cautioned against over-reliance on imaging. In their study 23 of 52 flaps (44%) underwent intraoperative changes due to features not noted on preoperative computed tomography. However, Rozen et al. [8], in a cadaveric study of 154 perforators in 10 hemiabdominal walls, revealed a sensitivity of 96% and positive predictive value of 95% when comparing CTA and surgical dissection measurements of perforators from an umbilical reference point. While CTA continues to serve as the gold standard in preoperative planning for perforator flaps, it is important for surgeons to rely foremost on their clinical judgment and use imaging as a supplement.
In the case presented, intraoperative surgical judgment transcended preoperative planning of the CTA. This case emphasizes the importance of a versatile reconstructive plan as well as clinical resilience in real-time. Although adequately sized muscular perforators were present, fibrotic tissue consequent of prior operations encased the DIEA bilaterally. These findings were not appreciated or adequately illustrated preoperatively on the CTA. Thus, this case illustrates the importance of an adaptable surgical plan based on individual aberrant anatomy.
Notes
No potential conflict of interest relevant to this article was reported.