INTRODUCTION
Progressive facial hemiatrophy, also known as Parry-Romberg syndrome, is a rare disease (1/700,000), which usually affects women. It begins in the first two decades of life; however, it has also been reported in the fifth or sixth decade with a mean age of presentation of 8.8 years. It is characterized by a progressive, self-limited deformation and reduction of the subcutaneous tissue volume on one side of the face, which involves scar-like skin changes, atrophy of the subcutaneous and adipose tissue, circumscribed osteoporosis, trigeminal neuralgia, and changes in the hair and eyes [1].
The first sign of this disease is thinning of the skin and subcutaneous tissue, often preceded by a discoloration of the hair or alopecia areata. It may also involve the mouth, nose or ear, and damage is usually limited to a trigeminal area and it usually does not cross the midline. The final result is a craniofacial asymmetry, which not only causes aesthetic discomfort, but also weakens self-esteem, affecting growth and intellectual development of the patient [2].
Throughout history many procedures have been described in an attempt to increase the volume lost by gradual atrophy of soft tissues: dermis-fat grafts, omental free flaps, and musculoskeletal free flaps, just to mention a few. Currently the use of a fat transfer to replenish volume is an increasingly popular method in the field of craniofacial surgery [3]. The introduction of liposuction and liposculpture techniques by Illouz [4] and Fournier and Otteni [5] was a milestone in the history of autologous fat transfer. Subsequently, Coleman [6] indicated that the reabsorption of injected fat is a constant and would require repeated injection. This led him to describe better methods for the aspiration, processing and application of fat, which includes thin cannulas, decantation, centrifugation, and filtration of the lipoaspirate.
Matsumoto et al. [7] described a technique called cell-assisted lipotransfer (CAL) that consists of an autologous adipose tissue transplant enriched with adipose-derived stem cells (ASCs). Using enzymatic digestion with collagenase and centrifugation a cell pellet known as the stromal vascular fraction (SVF) that contains stromal cells, endothelial progenitor cells, ASCs, preadipocytes, and is devoid of adipocytes, is used to enrich the fat graft to be injected.
ASCs from the SVF have several advantages: they can differentiate directly into adipocytes and contribute to adipose tissue regeneration, promote angiogenesis and survival of the graft through differentiation into endothelial cells, release angiogenic growth factors in response to injury and hypoxia and finally, some can survive as stem cells. Yoshimura et al. [8,9] used this technique in patients with facial lipoatrophy and cosmetic breasts augmentation with excellent results.
CASE
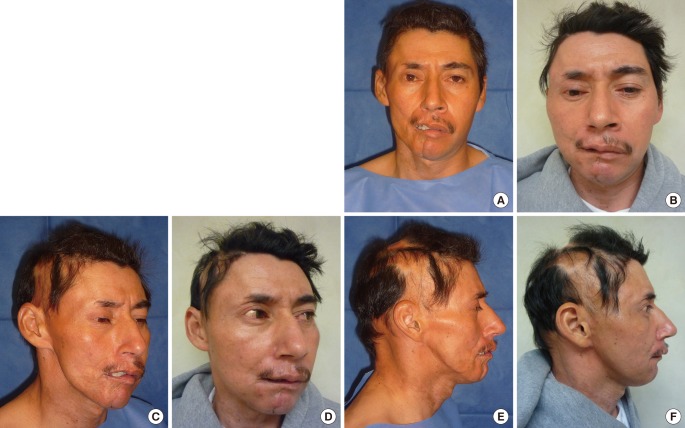
The patient is a 35-year-old man with no previous medical history, diagnosed with progressive right hemifacial atrophy of 10 years evolution and 5 years with a stabilized condition. On examination, alopecia was found in the parietal and temporal region, together with subcutaneous tissue atrophy of the temporal region and the right midface, tooth loss, decreased range of motion of the temporomandibular joint, and trigeminal neuralgia. Computed tomography with 3-dimensional (3D) reconstruction showed the absence of the temporomandibular joint and a significant reduction of tissue volume in the affected side.
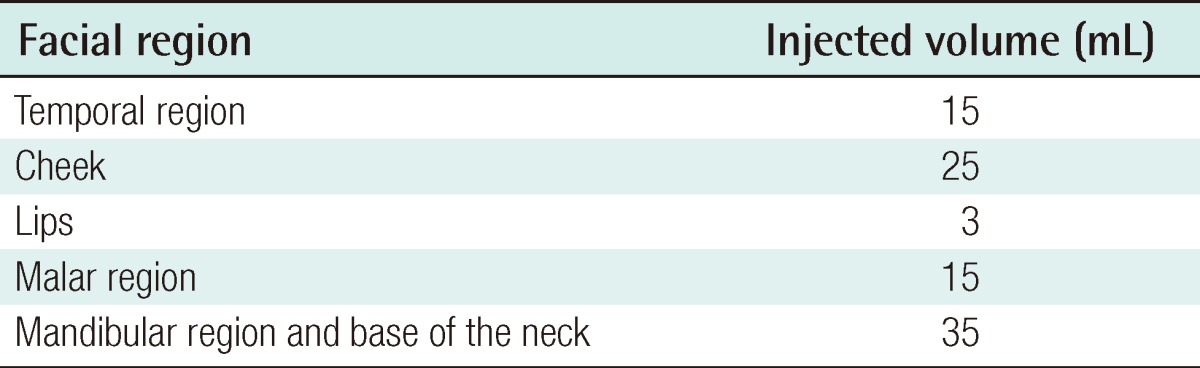
We preformed a previous analysis of the degree of atrophy marking the face with 18 squares using four horizontal planes crossed by seven vertical planes. This helped us identify the areas and volume to inject for facial volume replacement under general anesthesia. We infiltrated the skin with a tumescent Klein solution (solucion HT 1,000 mL with epinephrine 1 mg/mL, PiSA Farmaceutica Mexicana, SA de CV, Guadalajara, Mexico) in the periumbilical region and continued with fat extraction with a 3-mm blunt cannula connected to a 20 mL syringe. We extracted a total of 300 mL of fat, from which we separated 150 mL for processing and extraction of the ASCs. We followed the procedure described by Yoshimura et al. [8,9] (except for the isolation of stem cells from the fluid portion): digestion with collagenase, type II (Gibco, Invitrogen, Carlsbad, CA, USA) and centrifugation (800×g, 10 minutes), with a duration of approximately 90 minutes. With the resulting pellet we enriched the 150 mL initially separated. For injection we used 1 and 3 mL syringes connected to a 2-mm blunt cannula; 50% of the enriched fat was injected into the submuscular layer, and the remaining fat in the subcutaneous stratum (Table 1).
DISCUSSION
The postoperative evolution of our patient in the short and long term (1 and 12 months) was satisfactory (Fig. 1). Infiltration with enriched autologous fat containing ASCs reduced the severe depression of the frontotemporal region, and provided better volume and symmetry. An acceptable improvement of the malar prominence and cheek was also achieved, with greater volume and projection on the front view and profile. The contour of the mandibular border from the angle to the chin was redefined, achieving a better balance, even the neck base benefitted volumetrically. It is important to point out the permanence of the fat graft in the lips, which allows the teeth to be hidden because of the increase in lip volume. The permanence of the graft remained stable in all the injected areas, even in the nasolabial folds and lips, which are areas of maximum mobility and reabsorption.
Finally, from our point of view and also that of the patient, another important aspect with this technique, which has not been reported in the literature, is the clinical improvement of skin quality: better moisture, texture, shine, and even elasticity.
Soft tissue involvement in Parry-Romberg syndrome is global, including the craniofacial skeleton. It may have varying degrees of atrophy and hence the facial asymmetry is more evident. Although there is no treatment for the underlying etiology, clinical protocols with immunomodulatory drugs are being performed. Currently, we focus therapy on restoring volume and improving facial expressions.
The literature has reported better results when aspirated fat is processed with Coleman's method, which has less reabsorption and more predictable results. The use of autologous fat as a filler has been quite acceptable in patients with soft tissue atrophy, such as in Parry-Romberg syndrome. For this reason, we propose the combination of autologous fat transplant with SVF elements that contain ASCs. This technique could be considered standard treatment [10,11].
A larger study with more patients will provide the basis for understanding the involvement of ASCs, not only as an adjunct for tissue regeneration, but also for the skin itself. In the near future we consider that its use will be the beginning of a new treatment strategy for patients with different degrees of soft tissue atrophy.